

HIV Infection and Survival Among Women With Cervical Cancer
- PMID: 27573661
- PMCID: PMC5477924
- DOI: 10.1200/JCO.2016.67.9613
HIV Infection and Survival Among Women With Cervical Cancer
Abstract
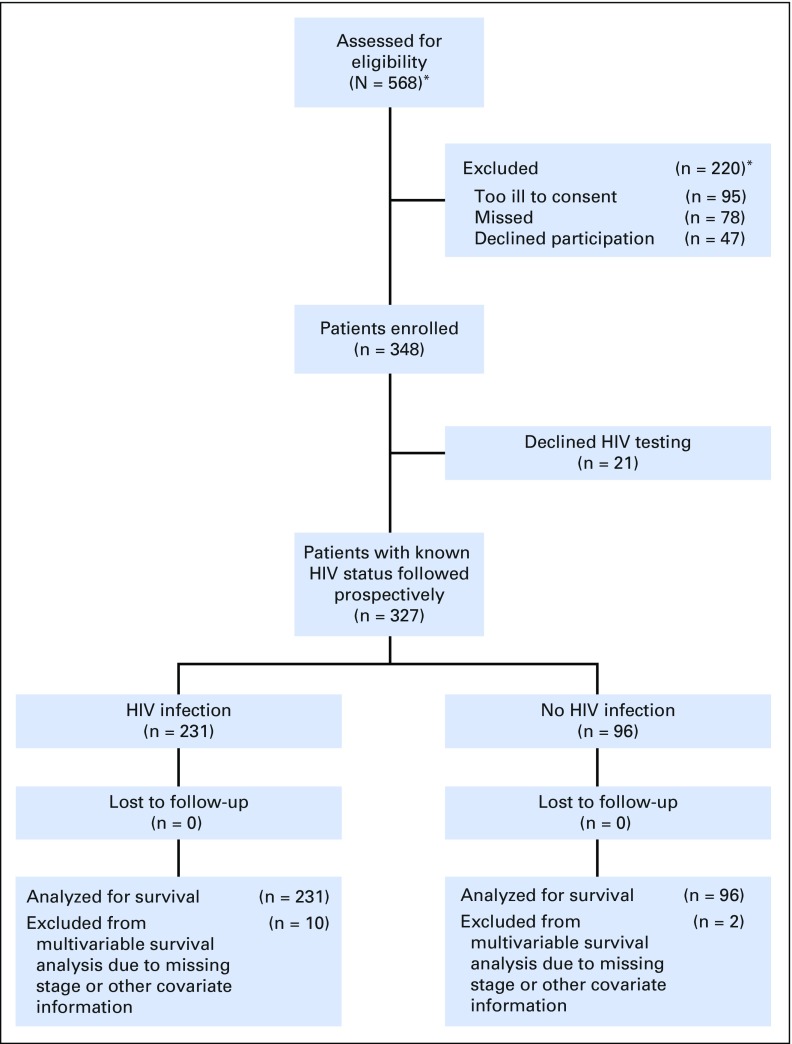
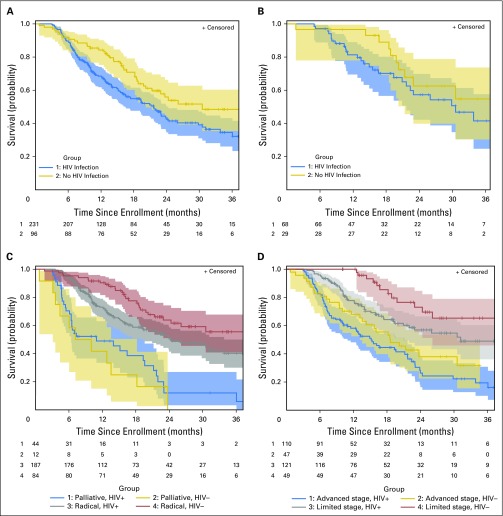
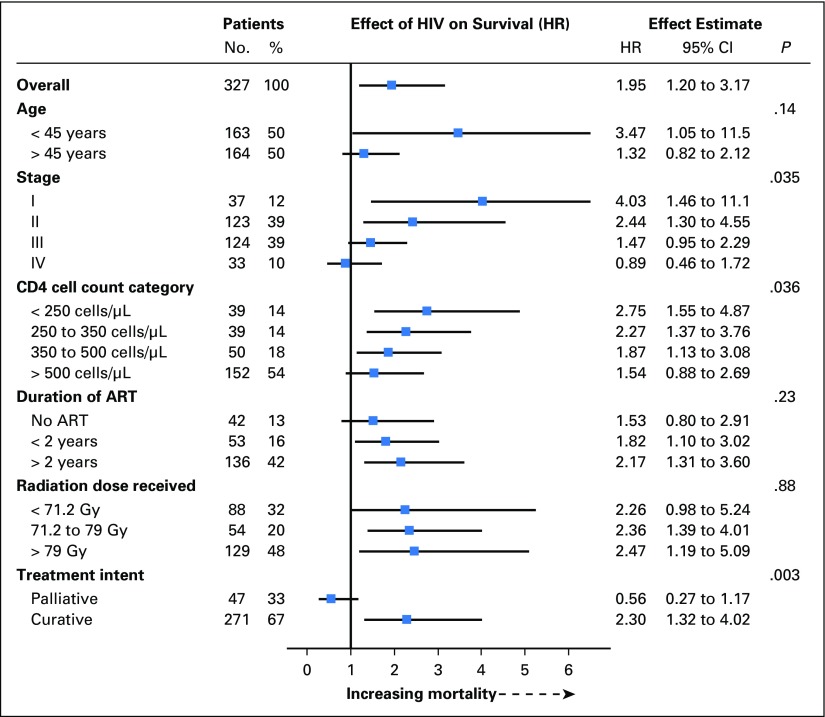
Purpose Cervical cancer is the leading cause of cancer death among the 20 million women with HIV worldwide. We sought to determine whether HIV infection affected survival in women with invasive cervical cancer. Patients and Methods We enrolled sequential patients with cervical cancer in Botswana from 2010 to 2015. Standard treatment included external beam radiation and brachytherapy with concurrent cisplatin chemotherapy. The effect of HIV on survival was estimated by using an inverse probability weighted marginal Cox model. Results A total of 348 women with cervical cancer were enrolled, including 231 (66.4%) with HIV and 96 (27.6%) without HIV. The majority (189 [81.8%]) of women with HIV received antiretroviral therapy before cancer diagnosis. The median CD4 cell count for women with HIV was 397 (interquartile range, 264 to 555). After a median follow-up of 19.7 months, 117 (50.7%) women with HIV and 40 (41.7%) without HIV died. One death was attributed to HIV and the remaining to cancer. Three-year survival for the women with HIV was 35% (95% CI, 27% to 44%) and 48% (95% CI, 35% to 60%) for those without HIV. In an adjusted analysis, HIV infection significantly increased the risk for death among all women (hazard ratio, 1.95; 95% CI, 1.20 to 3.17) and in the subset that received guideline-concordant curative treatment (hazard ratio, 2.63; 95% CI, 1.05 to 6.55). The adverse effect of HIV on survival was greater for women with a more-limited stage cancer ( P = .035), those treated with curative intent ( P = .003), and those with a lower CD4 cell count ( P = .036). Advanced stage and poor treatment completion contributed to high mortality overall. Conclusion In the context of good access to and use of antiretroviral treatment in Botswana, HIV infection significantly decreases cervical cancer survival.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at
Figures
Comment in
-
Improvement of Outcomes for Women With HIV Infection and Cervical Cancer.J Clin Oncol. 2016 Nov 1;34(31):3719-3721. doi: 10.1200/JCO.2016.69.0784. J Clin Oncol. 2016. PMID: 27573654 Free PMC article. No abstract available.
References
-
- Grulich AE, van Leeuwen MT, Falster MO, et al. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis. Lancet. 2007;370:59–67. - PubMed
-
- Blitz S, Baxter J, Raboud J, et al. Evaluation of HIV and highly active antiretroviral therapy on the natural history of human papillomavirus infection and cervical cytopathologic findings in HIV-positive and high-risk HIV-negative women. J Infect Dis. 2013;208:454–462. - PubMed
-
- Joint United National Programme on HIV/AIDS (UNAIDS). The Gap Report. Geneva, Switzerland, UNAIDS, 2014.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
