

Ultrasound guidance for lumbar puncture
- PMID: 27574571
- PMCID: PMC4987119
- DOI: 10.1212/CPJ.0000000000000265
Ultrasound guidance for lumbar puncture
Abstract
Purpose of review: To review the literature and describe techniques to use ultrasound to guide performance of lumbar puncture (LP).
Recent findings: Ultrasound evaluation of the lumbar spine has been shown in randomized trials to improve LP success rates while reducing the number of attempts and the number of traumatic taps.
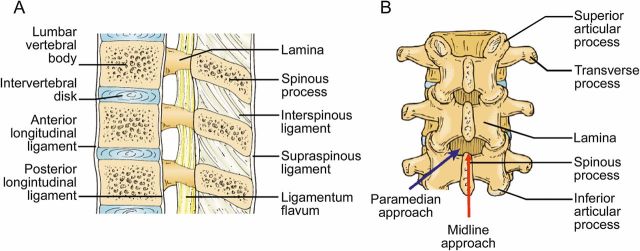
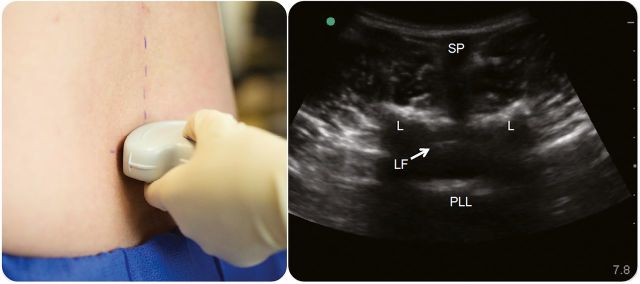
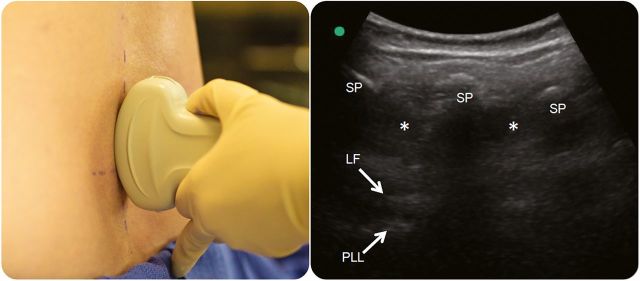
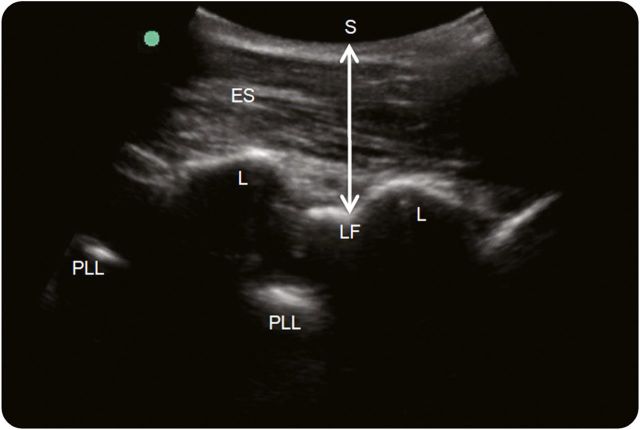
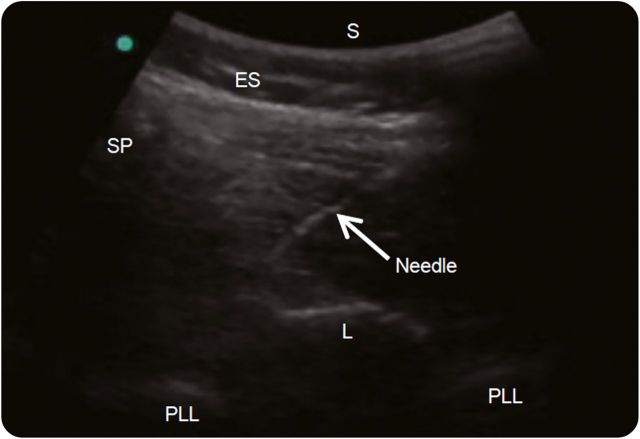
Summary: Ultrasound mapping of the lumbar spine reveals anatomical information that is not obtainable by physical examination, including depth of the ligamentum flavum, width of the interspinous spaces, and spinal bone abnormalities, including scoliosis. Using static ultrasound, the lumbar spine anatomy is visualized in transverse and longitudinal planes and the needle insertion site is marked. Using real-time ultrasound guidance, the needle tip is tracked in a paramedian plane as it traverses toward the ligamentum flavum. Future research should focus on efficient methods to train providers, cost-effectiveness of ultrasound-guided LP, and the role of new needle-tracking technologies to facilitate the procedure.
Figures
References
-
- Edwards C, Leira EC, Gonzalez-Alegre P. Residency training: a failed lumbar puncture is more about obesity than lack of ability. Neurology 2015;84:e69–e72. - PubMed
-
- Bogin IN, Stulin ID. Application of the method of 2-dimensional echospondylography for determining landmarks in lumbar punctures [in Russian]. Zh Nevropatol Psikhiatr Ime S S Korsakova 1971;71:1810–1811. - PubMed
-
- Grau T, Leipold R, Conradi R, Martin E, Motsch J. Ultrasonography and peridural anesthesia: technical possibilities and limitations of ultrasonic examination of the epidural space [in German]. Anaesthesist 2001;50:94–101. - PubMed
-
- Grau T, Leipold RW, Conradi R, Martin E. Ultrasound control for presumed difficult epidural puncture. Acta Anaesthesiol Scand 2001;45:766–771. - PubMed
-
- Grau T, Leipold RW, Horter J, Conradi R, Martin E, Motsch J. The lumbar epidural space in pregnancy: visualization by ultrasonography. Br J Anaesth 2001;86:798–804. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials