

Ultrafiltration Rate and Mortality in Maintenance Hemodialysis Patients
- PMID: 27575009
- PMCID: PMC5123913
- DOI: 10.1053/j.ajkd.2016.06.020
Ultrafiltration Rate and Mortality in Maintenance Hemodialysis Patients
Abstract
Background: Observational data have demonstrated an association between higher ultrafiltration rates and greater mortality among hemodialysis patients. Prior studies were small and did not consider potential differences in the association across body sizes and other related subgroups. No study has investigated ultrafiltration rates normalized to anthropometric measures beyond body weight. Also, potential methodological shortcomings in prior studies have led to questions about the veracity of the ultrafiltration rate-mortality association.
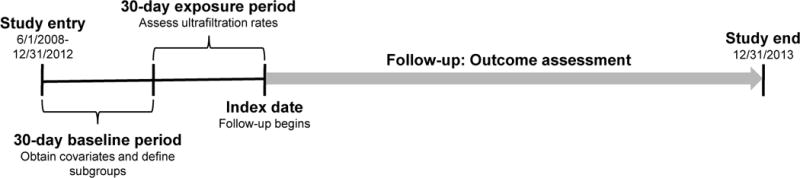
Study design: Retrospective cohort.
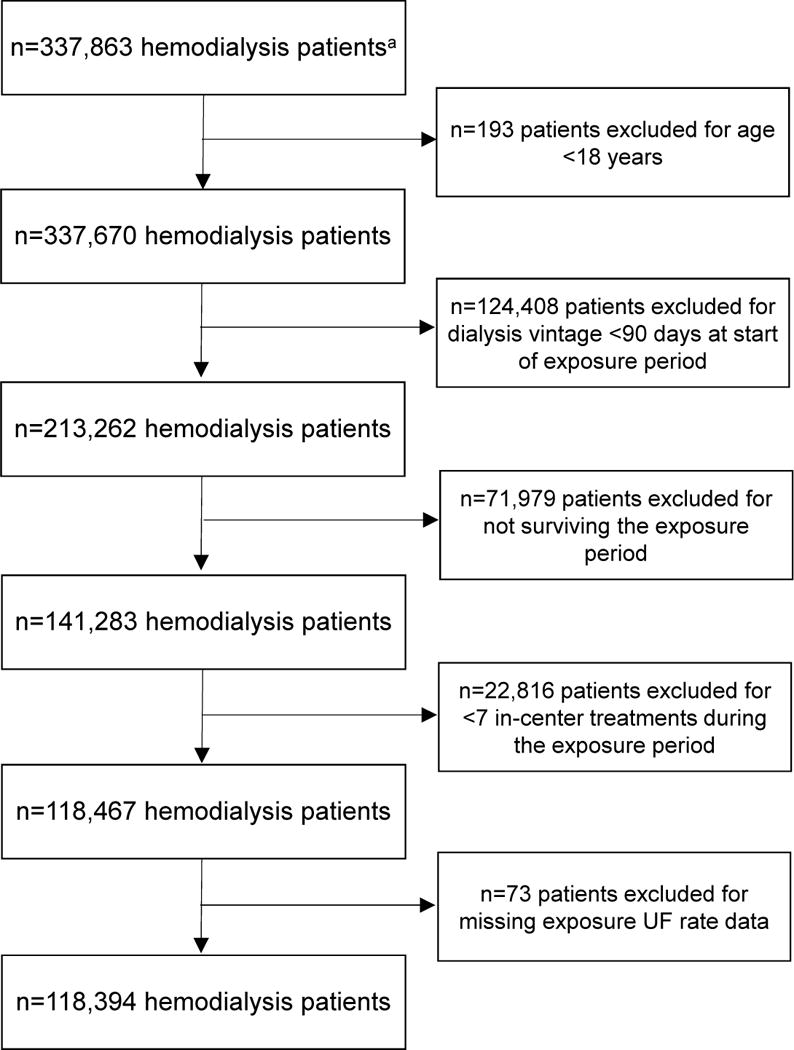
Setting & participants: 118,394 hemodialysis patients dialyzing in a large dialysis organization, 2008 to 2012.
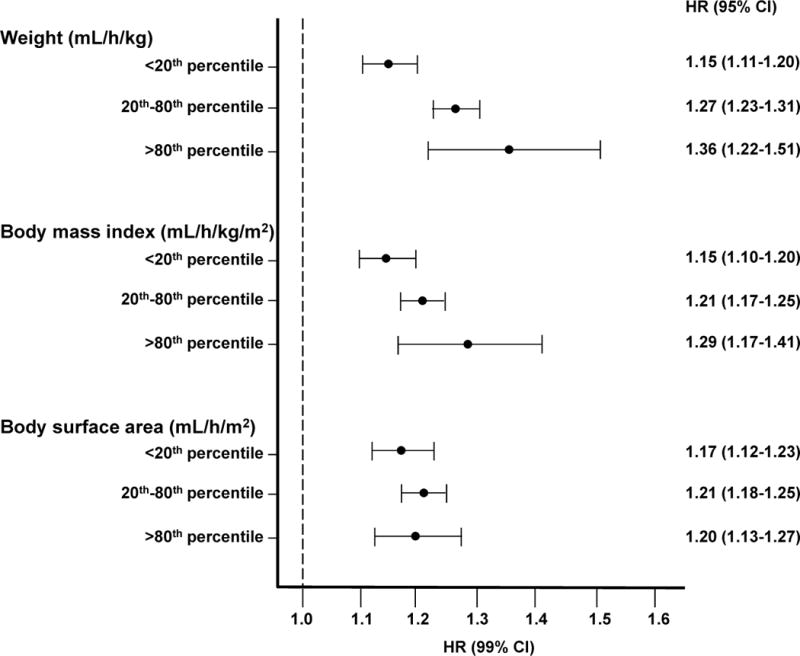
Predictors: Mean 30-day ultrafiltration rates were dichotomized at 13 and 10mL/h/kg, separately and categorized using various cutoff points. Ultrafiltration rates normalized to body weight, body mass index, and body surface area were investigated.
Outcomes: All-cause mortality.
Measurements: Multivariable survival models were used to estimate the association between ultrafiltration rate and all-cause mortality.
Results: At baseline, 21,735 (18.4%) individuals had ultrafiltration rates > 13mL/h/kg and 48,529 (41.0%) had ultrafiltration rates > 10mL/h/kg. Median follow-up was 2.3 years, and the mortality rate was 15.3 deaths/100 patient-years. Compared with ultrafiltration rates ≤ 13mL/h/kg, ultrafiltration rates > 13mL/h/kg were associated with greater mortality (adjusted HR, 1.31; 95% CI, 1.28-1.34). Compared with ultrafiltration rates ≤ 10mL/h/kg, ultrafiltration rates > 10mL/h/kg were associated with greater mortality (adjusted HR, 1.22; 95% CI, 1.20-1.24). Findings were consistent across subgroups of sex, race, dialysis vintage, session duration, and body size. Higher ultrafiltration rates were associated with greater mortality when normalized to body weight, body mass index, and body surface area.
Limitations: Residual confounding cannot be excluded given the observational study design.
Conclusions: Regardless of the threshold implemented, higher ultrafiltration rate was associated with greater mortality in the overall study population and across key subgroups. Randomized controlled trials are needed to investigate whether ultrafiltration rate reduction improves clinical outcomes.
Keywords: Hemodialysis; anthropometric measures; body mass index (BMI); body size; body surface area (BSA); body weight; end-stage renal disease (ESRD); metabolic mass; mortality; rapid fluid removal; ultrafiltration rate (UFR).
Copyright © 2016 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Collins AJ, Foley RN, Chavers B, et al. US Renal Data System 2013 annual data report. Am J Kidney Dis. 2014;63(1 (suppl 1)):e1–e420. - PubMed
-
- Saran R, Bragg-Gresham JL, Levin NW, et al. Longer treatment time and slower ultrafiltration in hemodialysis: associations with reduced mortality in the DOPPS. Kidney Int. 2006;69(7):1222–1228. - PubMed
-
- Movilli E, Gaggia P, Zubani R, et al. Association between high ultrafiltration rates and mortality in uraemic patients on regular haemodialysis. A 5-year prospective observational multicentre study. Nephrol Dial Transplant. 2007;22(12):3547–3552. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
