

An Audit and Feedback Intervention for Reducing Antibiotic Prescribing in General Dental Practice: The RAPiD Cluster Randomised Controlled Trial
- PMID: 27575599
- PMCID: PMC5004857
- DOI: 10.1371/journal.pmed.1002115
An Audit and Feedback Intervention for Reducing Antibiotic Prescribing in General Dental Practice: The RAPiD Cluster Randomised Controlled Trial
Abstract
Background: Dentists prescribe approximately 10% of antibiotics dispensed in UK community pharmacies. Despite clear clinical guidance, dentists often prescribe antibiotics inappropriately. This cluster-randomised controlled trial used routinely collected National Health Service (NHS) dental prescribing and treatment claim data to compare the impact of individualised audit and feedback (A&F) interventions on dentists' antibiotic prescribing rates.
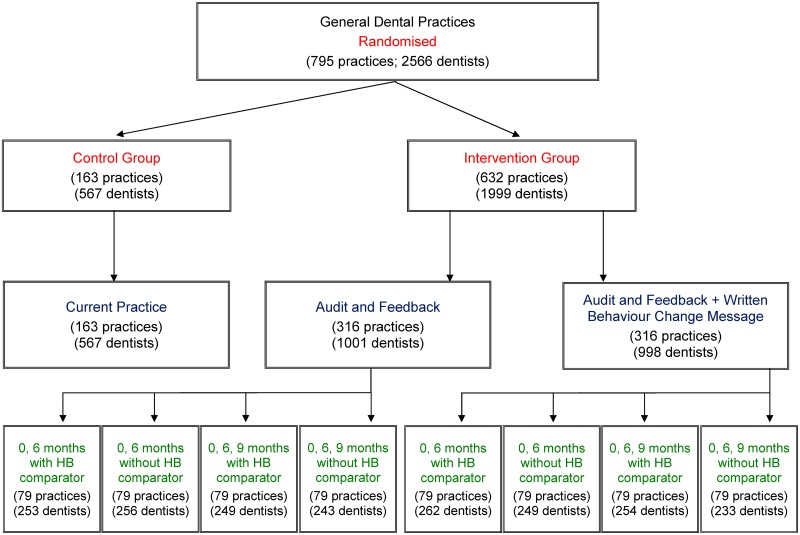
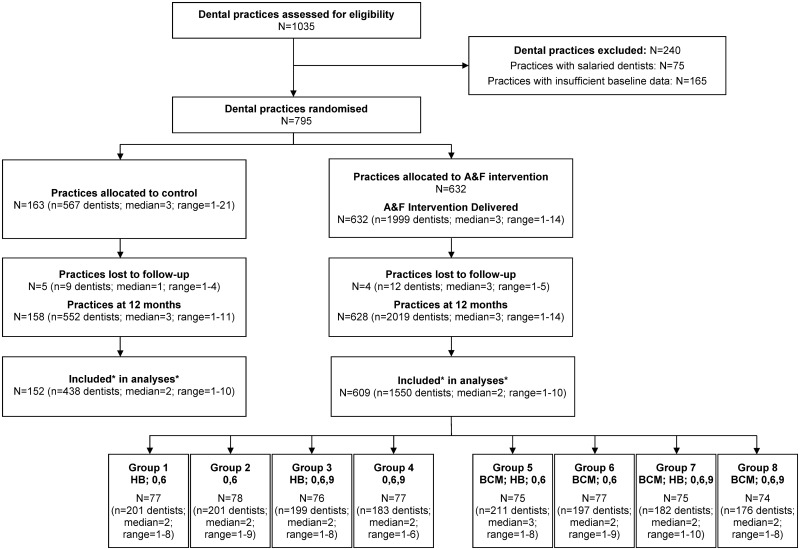
Methods and findings: All 795 antibiotic prescribing NHS general dental practices in Scotland were included. Practices were randomised to the control (practices = 163; dentists = 567) or A&F intervention group (practices = 632; dentists = 1,999). A&F intervention practices were allocated to one of two A&F groups: (1) individualised graphical A&F comprising a line graph plotting an individual dentist's monthly antibiotic prescribing rate (practices = 316; dentists = 1,001); or (2) individualised graphical A&F plus a written behaviour change message synthesising and reiterating national guidance recommendations for dental antibiotic prescribing (practices = 316; dentists = 998). Intervention practices were also simultaneously randomised to receive A&F: (i) with or without a health board comparator comprising the addition of a line to the graphical A&F plotting the monthly antibiotic prescribing rate of all dentists in the health board; and (ii) delivered at 0 and 6 mo or at 0, 6, and 9 mo, giving a total of eight intervention groups. The primary outcome, measured by the trial statistician who was blinded to allocation, was the total number of antibiotic items dispensed per 100 NHS treatment claims over the 12 mo post-delivery of the baseline A&F. Primary outcome data was available for 152 control practices (dentists = 438) and 609 intervention practices (dentists = 1,550). At baseline, the number of antibiotic items prescribed per 100 NHS treatment claims was 8.3 in the control group and 8.5 in the intervention group. At follow-up, antibiotic prescribing had decreased by 0.4 antibiotic items per 100 NHS treatment claims in control practices and by 1.0 in intervention practices. This represents a significant reduction (-5.7%; 95% CI -10.2% to -1.1%; p = 0.01) in dentists' prescribing rate in the intervention group relative to the control group. Intervention subgroup analyses found a 6.1% reduction in the antibiotic prescribing rate of dentists who had received the written behaviour change message relative to dentists who had not (95% CI -10.4% to -1.9%; p = 0.01). There was no significant between-group difference in the prescribing rate of dentists who received a health board comparator relative to those who did not (-4.3%; 95% CI -8.6% to 0.1%; p = 0.06), nor between dentists who received A&F at 0 and 6 mo relative to those who received A&F at 0, 6, and 9 mo (0.02%; 95% CI -4.2% to 4.2%; p = 0.99). The key limitations relate to the use of routinely collected datasets which did not allow evaluation of any effects on inappropriate prescribing.
Conclusions: A&F derived from routinely collected datasets led to a significant reduction in the antibiotic prescribing rate of dentists.
Trial registration: Current Controlled Trials ISRCTN49204710.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: Authors LY and JEC are employed by NHS Education for Scotland, which is responsible for supporting NHS services in Scotland by developing and delivering education and training for those who work in NHS Scotland. Author AE declared that during the course of the study, he was in paid full-time employment firstly by the University of Aberdeen and subsequently by Glasgow Caledonian University. The research was carried out on behalf of the TRiaDS Research Methodology Group (of which AE is a member). This group is funded by NHS Education for Scotland. No other competing interests exist.
Figures
References
-
- World Health Organisation. Antimicrobial resistance: global report on surveillance. 2014. http://www.who.int/drugresistance/documents/surveillancereport/en/.
-
- Goossens H, Ferech M, Vander Stichele R, Elseviers M, for the ESAC Project Group. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet. 2005;365(9459):579–587. - PubMed
-
- Martin MV. Antimicrobials and dentistry: a rationale for their use. Fac Dent J. 2010;1:15–19.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
