

Middle East Respiratory Syndrome: Emergence of a Pathogenic Human Coronavirus
- PMID: 27576010
- PMCID: PMC5353356
- DOI: 10.1146/annurev-med-051215-031152
Middle East Respiratory Syndrome: Emergence of a Pathogenic Human Coronavirus
Abstract
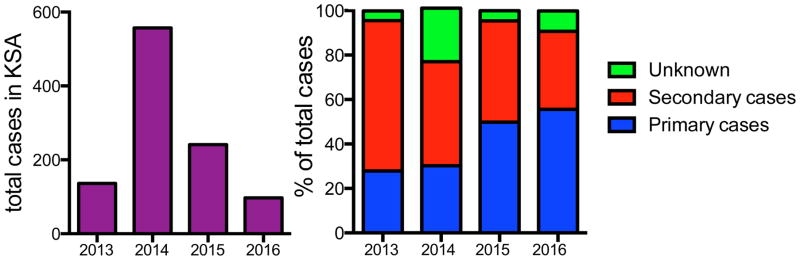
In 2012, a zoonotic coronavirus was identified as the causative agent of Middle East respiratory syndrome and was named MERS coronavirus (MERS-CoV). As of August 11, 2016, the virus has infected 1,791 patients, with a mortality rate of 35.6%. Although MERS-CoV generally causes subclinical or mild disease, infection can result in serious outcomes, including acute respiratory distress syndrome and multi-organ failure in patients with comorbidities. The virus is endemic in camels in the Arabian Peninsula and Africa and thus poses a consistent threat of frequent reintroduction into human populations. Disease prevalence will increase substantially if the virus mutates to increase human-to-human transmissibility. No therapeutics or vaccines are approved for MERS; thus, development of novel therapies is needed. Further, since many MERS cases are acquired in healthcare settings, public health measures and scrupulous attention to infection control are required to prevent additional MERS outbreaks.
Keywords: animal models; antiviral therapies; camels; host–virus interactions; immune response; outbreak.
Figures
References
-
- Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. The New England journal of medicine. 2012;367:1814–20. - PubMed
-
- Lee SS, Wong NS. Probable transmission chains of Middle East respiratory syndrome coronavirus and the multiple generations of secondary infection in South Korea. International journal of infectious diseases: IJID: official publication of the International Society for Infectious Diseases. 2015;38:65–7. - PMC - PubMed
-
- Masters PS, Perlman S. Coronaviridae. In: Howley PM, Knipe DM, editors. Fields Virology. Vol. 6. Philadelphia, PA: Lippincott Williams and Wilkins, a Wolters Kluwer business; 2013. pp. 825–58.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
