

Long-term survival in AIDS-related primary central nervous system lymphoma
- PMID: 27576871
- PMCID: PMC5193026
- DOI: 10.1093/neuonc/now155
Long-term survival in AIDS-related primary central nervous system lymphoma
Abstract
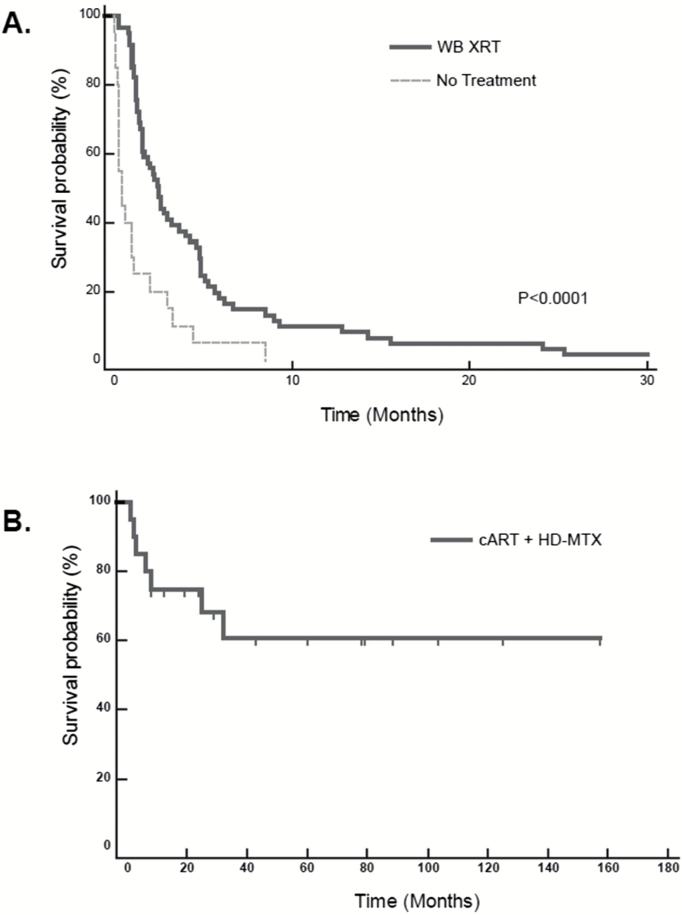
Background: The optimal therapeutic approach for patients with AIDS-related primary central nervous system lymphoma (AR-PCNSL) remains undefined. While its incidence declined substantially with combination antiretroviral therapy (cART), AR-PCNSL remains a highly aggressive neoplasm for which whole brain radiotherapy (WBRT) is considered a standard first-line intervention.
Methods: To identify therapy-related factors associated with favorable survival, we first retrospectively analyzed outcomes of AR-PCNSL patients treated at San Francisco General Hospital, a public hospital with a long history of dedicated care for patients with HIV and AIDS-related malignancies. Results were validated in a retrospective, multicenter analysis that evaluated all newly diagnosed patients with AR-PCNSL treated with cART plus high-dose methotrexate (HD-MTX).
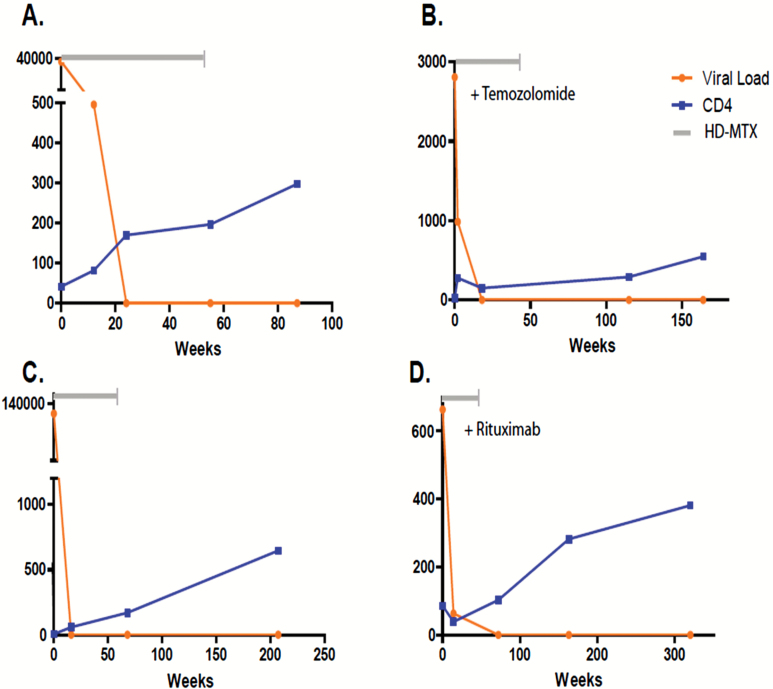
Results: We provide evidence that CD4+ reconstitution with cART administered during HD-MTX correlates with long-term survival among patients with CD4 <100. This was confirmed in a multicenter analysis which demonstrated that integration of cART regimens with HD-MTX was generally well tolerated and resulted in longer progression-free survival than other treatments. No profound differences in immunophenotype were identified in an analysis of AR-PCNSL tumors that arose in the pre- versus post-cART eras. However, we detected evidence for a demographic shift, as the proportion of minority patients with AR-PCNSL increased since advent of cART.
Conclusion: Long-term disease-free survival can be achieved in AR-PCNSL, even among those with histories of opportunistic infections, limited access to health care, and medical non-adherence. Given this, as well as the long-term toxicities of WBRT, we recommend that integration of cART plus first-line HD-MTX be considered for all patients with AR-PCNSL.
Keywords: AIDS; HAART; brain tumor; lymphoma; methotrexate.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Long-term AIDS-related PCNSL outcomes with HD-MTX and combined antiretroviral therapy.Neurology. 2017 Aug 22;89(8):796-804. doi: 10.1212/WNL.0000000000004265. Epub 2017 Jul 26. Neurology. 2017. PMID: 28747447
-
Stereotactic radiosurgery in combination with up-front high-dose methotrexate as a first-line treatment for newly diagnosed primary central nervous system lymphoma.J Neurooncol. 2015 Jun;123(2):237-44. doi: 10.1007/s11060-015-1786-1. Epub 2015 Apr 25. J Neurooncol. 2015. PMID: 25911295
-
A prospective phase II trial of response adapted whole brain radiotherapy after high dose methotrexate based chemotherapy in patients with newly diagnosed primary central nervous system lymphoma-analysis of acute toxicity profile and early clinical outcome.J Neurooncol. 2018 Aug;139(1):153-166. doi: 10.1007/s11060-018-2856-y. Epub 2018 Apr 9. J Neurooncol. 2018. PMID: 29633112 Clinical Trial.
-
High-dose methotrexate-based chemotherapy for induction remission of newly diagnosed primary CNS lymphoma: A systematic review and meta-analysis.Medicine (Baltimore). 2025 Jan 31;104(5):e41363. doi: 10.1097/MD.0000000000041363. Medicine (Baltimore). 2025. PMID: 39889167 Free PMC article.
-
[Primary central nervous system lymphoma--a report of 32 cases with literature review].Ai Zheng. 2006 Apr;25(4):476-80. Ai Zheng. 2006. PMID: 16613684 Review. Chinese.
Cited by
-
A multicenter, real-world analysis of primary central nervous system lymphoma in those with and without human immunodeficiency virus.EJHaem. 2022 Jun 2;3(3):734-738. doi: 10.1002/jha2.474. eCollection 2022 Aug. EJHaem. 2022. PMID: 36051081 Free PMC article. No abstract available.
-
Primary central nervous system lymphoma: a real-world comparison of therapy access and outcomes by hospital setting.Neurooncol Pract. 2022 Jan 12;9(3):183-192. doi: 10.1093/nop/npab066. eCollection 2022 May. Neurooncol Pract. 2022. PMID: 35601974 Free PMC article.
-
Prognostic factors and surgical approaches in the analysis of primary central nervous system diffuse large B-cell lymphoma: a large population-based cohort study and external validation.Front Neurol. 2024 Nov 28;15:1431614. doi: 10.3389/fneur.2024.1431614. eCollection 2024. Front Neurol. 2024. PMID: 39677856 Free PMC article.
-
Long-term remission of AIDS-related primary central nervous system lymphoma in a patient under antiretroviral therapy: a case report and review of the literature.AIDS Res Ther. 2021 Oct 19;18(1):76. doi: 10.1186/s12981-021-00403-6. AIDS Res Ther. 2021. PMID: 34666791 Free PMC article. Review.
-
Distinct epigenetic and transcriptional profiles of Epstein-Barr virus-positive and negative primary CNS lymphomas.Neuro Oncol. 2025 May 15;27(4):979-992. doi: 10.1093/neuonc/noae251. Neuro Oncol. 2025. PMID: 39575767
References
-
- Levine AM. Acquired immunodeficiency syndrome-related lymphoma. Blood. 1992;80(1):8–20. - PubMed
-
- Forsyth PA, DeAngelis LM. Biology and management of AIDS-associated primary CNS lymphomas. Hematol Oncol Clin North Am. 1996;10(5):1125–34. - PubMed
-
- Raez LE, Patel P, Feun L. Natural history and prognostic factors for survival in patients with acquired immune deficiency syndrome (AIDS)-related primary central nervous system lymphoma (PCNSL). Crit Rev Oncog. 1998;9(3–4):199–208. - PubMed
-
- Fine HA, Mayer RJ. Primary central nervous system lymphoma. Ann Intern Med. 1993;119(11):1093–104. - PubMed
-
- Corn BW, Marcus SM, Topham A. Will primary central nervous system lymphoma be the most frequent brain tumor diagnosed in the year 2000? Cancer. 1997;79(12):2409–13. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
