

Is poor oral health a risk marker for incident cardiovascular disease hospitalisation and all-cause mortality? Findings from 172 630 participants from the prospective 45 and Up Study
- PMID: 27577588
- PMCID: PMC5013478
- DOI: 10.1136/bmjopen-2016-012386
Is poor oral health a risk marker for incident cardiovascular disease hospitalisation and all-cause mortality? Findings from 172 630 participants from the prospective 45 and Up Study
Abstract
Objective: To investigate the relationship between oral health and incident hospitalisation for ischaemic heart disease (IHD), heart failure (HF), ischaemic stroke and peripheral vascular disease (PVD) and all-cause mortality.
Design: Prospective population-based study of Australian men and women aged 45 years or older, who were recruited to the 45 and Up Study between January 2006 and April 2009; baseline questionnaire data were linked to hospitalisations and deaths up to December 2011. Study exposures include tooth loss and self-rated health of teeth and gums at baseline.
Setting: New South Wales, Australia.
Participants: Individuals aged 45-75 years, excluding those with a history of cancer/cardiovascular disease (CVD) at baseline; n=172 630.
Primary outcomes: Incident hospitalisation for IHD, HF, ischaemic stroke and PVD and all-cause mortality.
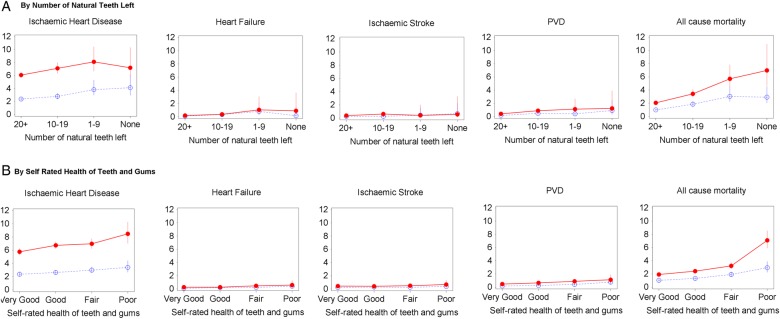
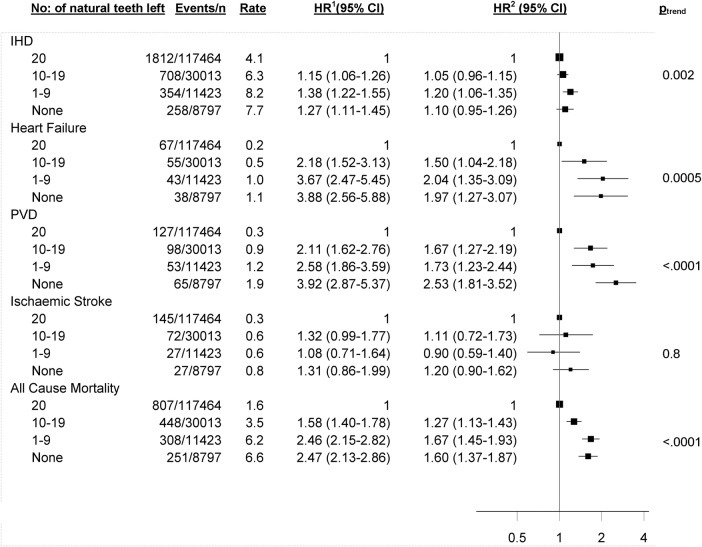
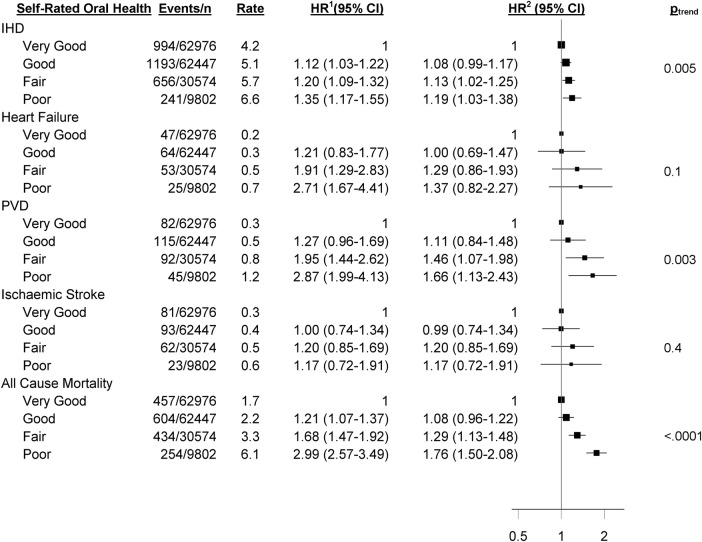
Results: During a median follow-up of 3.9 years, 3239 incident hospitalisations for IHD, 212 for HF, 283 for ischaemic stroke and 359 for PVD, and 1908 deaths, were observed. Cox proportional hazards models examined the relationship between oral health indicators and incident hospitalisation for CVD and all-cause mortality, adjusting for potential confounding factors. All-cause mortality and incident CVD hospitalisation risk increased significantly with increasing tooth loss for all outcomes except ischaemic stroke (ptrend<0.05). In those reporting no teeth versus ≥20 teeth left, risks were increased for HF (HR, 95% CI 1.97, 1.27 to 3.07), PVD (2.53, 1.81 to 3.52) and all-cause mortality (1.60, 1.37 to 1.87). The risk of IHD, PVD and all-cause mortality (but not HF or ischaemic stroke) increased significantly with worsening self-rated health of teeth and gums (ptrend<0.05). In those reporting poor versus very good health of teeth and gums, risks were increased for IHD (1.19, 1.03 to 1.38), PVD (1.66, 1.13 to 2.43) and all-cause mortality (1.76, 1.50 to 2.08).
Conclusions: Tooth loss and, to a lesser extent, self-rated health of teeth and gums, are markers for increased risk of IHD, PVD and all-cause mortality. Tooth loss is also a marker for increased risk of HF.
Keywords: cardiovascular disease epidemiology; mortality; oral health.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
 ; female:
; female:  .
.
Similar articles
-
Body mass index and incident hospitalisation for cardiovascular disease in 158 546 participants from the 45 and Up Study.Int J Obes (Lond). 2014 Jun;38(6):848-56. doi: 10.1038/ijo.2013.192. Epub 2013 Oct 23. Int J Obes (Lond). 2014. PMID: 24149770 Free PMC article.
-
Tooth Loss Predicts Myocardial Infarction, Heart Failure, Stroke, and Death.J Dent Res. 2019 Feb;98(2):164-170. doi: 10.1177/0022034518814829. J Dent Res. 2019. PMID: 30782090
-
Erectile dysfunction severity as a risk marker for cardiovascular disease hospitalisation and all-cause mortality: a prospective cohort study.PLoS Med. 2013;10(1):e1001372. doi: 10.1371/journal.pmed.1001372. Epub 2013 Jan 29. PLoS Med. 2013. PMID: 23382654 Free PMC article.
-
Bidirectional association between cardiovascular disease and hip fracture: a systematic review and meta-analysis.BMC Cardiovasc Disord. 2025 May 15;25(1):366. doi: 10.1186/s12872-025-04823-4. BMC Cardiovasc Disord. 2025. PMID: 40369408 Free PMC article.
-
The multifaceted impact of missing teeth on general health: A narrative review.Folia Med Cracov. 2024 Jun 30;64(1):25-37. doi: 10.24425/fmc.2024.150139. Folia Med Cracov. 2024. PMID: 39254579 Review.
Cited by
-
An Orthopedic Surgeon's Dental Examination: Reducing Unnecessary Delays in Joint Replacement Surgery for Marginalized Patients in a Safety Net Hospital System.Arthroplast Today. 2021 Nov 5;12:76-81. doi: 10.1016/j.artd.2021.10.001. eCollection 2021 Dec. Arthroplast Today. 2021. PMID: 34805467 Free PMC article.
-
Periodontal Diseases and Heart Diseases: A Systemic Review.J Pharm Bioallied Sci. 2023 Jul;15(Suppl 1):S72-S78. doi: 10.4103/jpbs.jpbs_517_22. Epub 2023 Jul 5. J Pharm Bioallied Sci. 2023. PMID: 37654288 Free PMC article.
-
Validity of the self-reported number of teeth in Chilean adults.BMC Oral Health. 2019 Jun 4;19(1):99. doi: 10.1186/s12903-019-0794-5. BMC Oral Health. 2019. PMID: 31164110 Free PMC article.
-
Risk of incident cardiovascular disease in people with periodontal disease: A systematic review and meta-analysis.Clin Exp Dent Res. 2021 Feb;7(1):109-122. doi: 10.1002/cre2.336. Epub 2020 Oct 30. Clin Exp Dent Res. 2021. PMID: 33124761 Free PMC article.
-
Association between gingivitis, tooth loss and cardiovascular risk: Insights from a 10-year nationwide cohort study of 3.7 million Koreans.PLoS One. 2024 Aug 2;19(8):e0308250. doi: 10.1371/journal.pone.0308250. eCollection 2024. PLoS One. 2024. PMID: 39093905 Free PMC article.
References
-
- Helfand M, Buckley DI, Freeman M et al. . Emerging risk factors for coronary heart disease: a summary of systematic reviews conducted for the U.S. Preventive Services Task Force. Ann Intern Med 2009;151:496–507. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous