

Impact of Preemptive Analgesia on inflammatory responses and Rehabilitation after Primary Total Knee Arthroplasty: A Controlled Clinical Study
- PMID: 27578313
- PMCID: PMC5005994
- DOI: 10.1038/srep30354
Impact of Preemptive Analgesia on inflammatory responses and Rehabilitation after Primary Total Knee Arthroplasty: A Controlled Clinical Study
Abstract
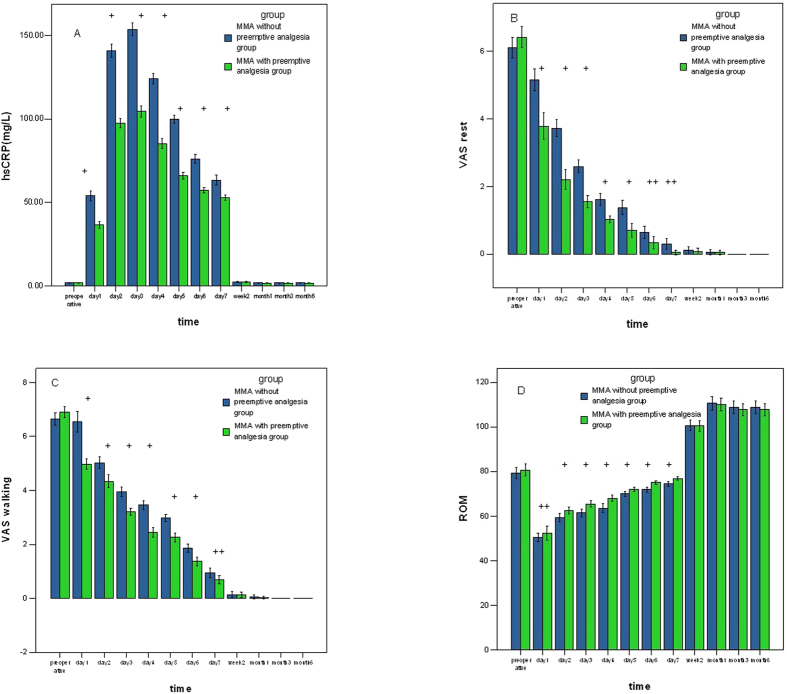
The aim of this study was to investigate the effects of preemptive analgesia on the inflammatory response and rehabilitation in TKA. 75 patients with unilateral primary knee osteoarthritis were conducted in this prospective study. All patients were randomly divided into two groups (MMA with/without preemptive analgesia group). The following parameters were used to evaluate analgesic efficacy: knee flexion, pain at rest and walking, functional walking capacity (2 MWT and 6 MWT), WOMAC score, and hs-CRP level. Patients in MMA with preemptive analgesia group had lower hs-CRP level and less pain at rest and walking during the first week postoperatively (P < 0.05). The 2 MWT was significantly better in MMA with preemptive analgesia group (17.13 ± 3.82 VS 14.19 ± 3.56, P = 0.001). The 6 MWT scores and WOMAC scores increased significantly within Groups (P = 0.020, 0.000), but no difference between groups postoperatively (P > 0.05). Less cumulative consumption of morphine was found in MMA with preemptive analgesia group at 48 h (P = 0.017, 0.023), but no difference at total requirement (P = 0.113). Preemptive analgesia added to a multimodal analgesic regime improved analgesia, reduced inflammatory reaction and accelerated functional recovery at the first week postoperatively, but not improved long-term function.
Figures
Similar articles
-
Role of Parecoxib Sodium in the Multimodal Analgesia after Total Knee Arthroplasty: A Randomized Double-blinded Controlled Trial.Orthop Surg. 2018 Nov;10(4):321-327. doi: 10.1111/os.12410. Orthop Surg. 2018. PMID: 30485685 Free PMC article. Clinical Trial.
-
Local infiltration analgesia versus intrathecal morphine for postoperative pain management after total knee arthroplasty: a randomized controlled trial.Anesth Analg. 2011 Oct;113(4):926-33. doi: 10.1213/ANE.0b013e3182288deb. Epub 2011 Aug 4. Anesth Analg. 2011. PMID: 21821506 Clinical Trial.
-
Perioperative pregabalin does not reduce opioid requirements in total knee arthroplasty.Knee Surg Sports Traumatol Arthrosc. 2019 Jul;27(7):2104-2110. doi: 10.1007/s00167-019-05385-7. Epub 2019 Feb 9. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 30739128 Clinical Trial.
-
Analgesia and functional outcome after total knee arthroplasty: periarticular infiltration vs continuous femoral nerve block.Br J Anaesth. 2010 Aug;105(2):185-95. doi: 10.1093/bja/aeq112. Epub 2010 Jun 14. Br J Anaesth. 2010. PMID: 20551021 Clinical Trial.
-
Postoperative pain management and proinflammatory cytokines: animal and human studies.J Neuroimmune Pharmacol. 2006 Dec;1(4):443-51. doi: 10.1007/s11481-006-9043-1. Epub 2006 Sep 29. J Neuroimmune Pharmacol. 2006. PMID: 18040817 Review.
Cited by
-
Efficacy of pre-emptive use of cyclooxyenase-2 inhibitors for total knee arthroplasty: a mini-review.Arthroplasty. 2019 Nov 27;1(1):13. doi: 10.1186/s42836-019-0015-3. Arthroplasty. 2019. PMID: 35240772 Free PMC article. Review.
-
Postoperative effect of sufentanil preemptive analgesia combined with psychological intervention on breast cancer patients.BMC Anesthesiol. 2023 May 20;23(1):170. doi: 10.1186/s12871-023-02143-8. BMC Anesthesiol. 2023. PMID: 37210488 Free PMC article. Clinical Trial.
-
The efficacy of pre-emptive analgesia on pain management in total knee arthroplasty: a mini-review.Arthroplasty. 2019 Oct 22;1(1):10. doi: 10.1186/s42836-019-0011-7. Arthroplasty. 2019. PMID: 35240765 Free PMC article. Review.
-
Risk factors and trajectories of opioid use following total knee replacement.Knee Surg Relat Res. 2022 Apr 5;34(1):18. doi: 10.1186/s43019-022-00148-0. Knee Surg Relat Res. 2022. PMID: 35382897 Free PMC article.
-
Combined Application of Dexamethasone and Tranexamic Acid to Reduce the Postoperative Inflammatory Response and Improve Functional Outcomes in Total Hip Arthroplasty.Orthop Surg. 2020 Apr;12(2):582-588. doi: 10.1111/os.12664. Orthop Surg. 2020. PMID: 32347005 Free PMC article. Clinical Trial.
References
-
- Rodriguez J. A., Bhende H. & Ranawat C. S. Total condylar knee replacement:a 20-year followup study. Clin Orthop Relat Res. 388, 10–17 (2001). - PubMed
-
- Capdevila X. et al.. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology. 91(1), 8–15 (1999). - PubMed
-
- Ranawat C. S., Ranawat A. S. & Mehta A. Total knee arthroplasty rehabilitation protocol: what makes the difference? J Arthroplasty. 18(1)(Suppl 1), 27–30 (2003). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
