

Epidemiology and Management of the 2013-16 West African Ebola Outbreak
- PMID: 27578439
- PMCID: PMC7297506
- DOI: 10.1146/annurev-virology-110615-040056
Epidemiology and Management of the 2013-16 West African Ebola Outbreak
Abstract
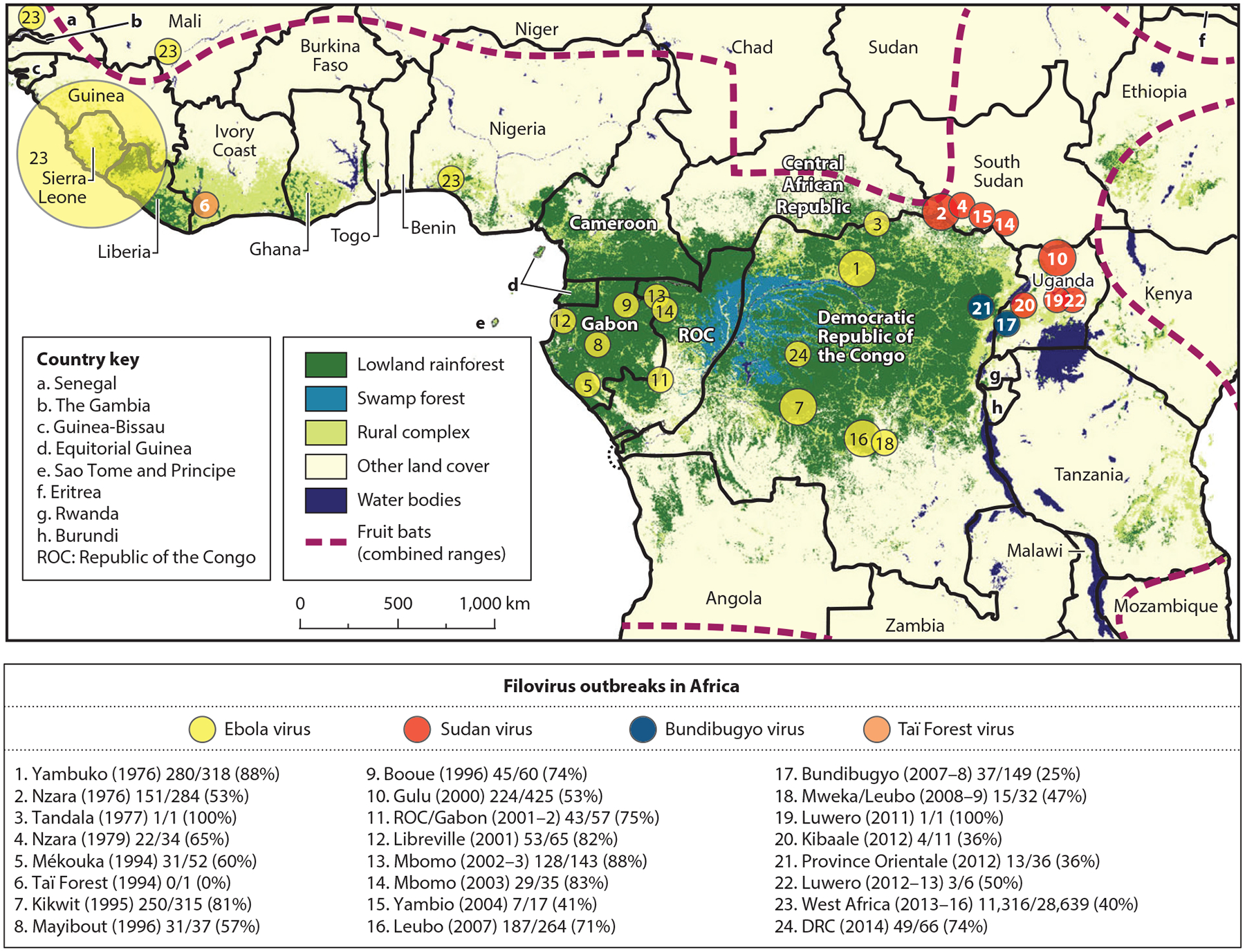
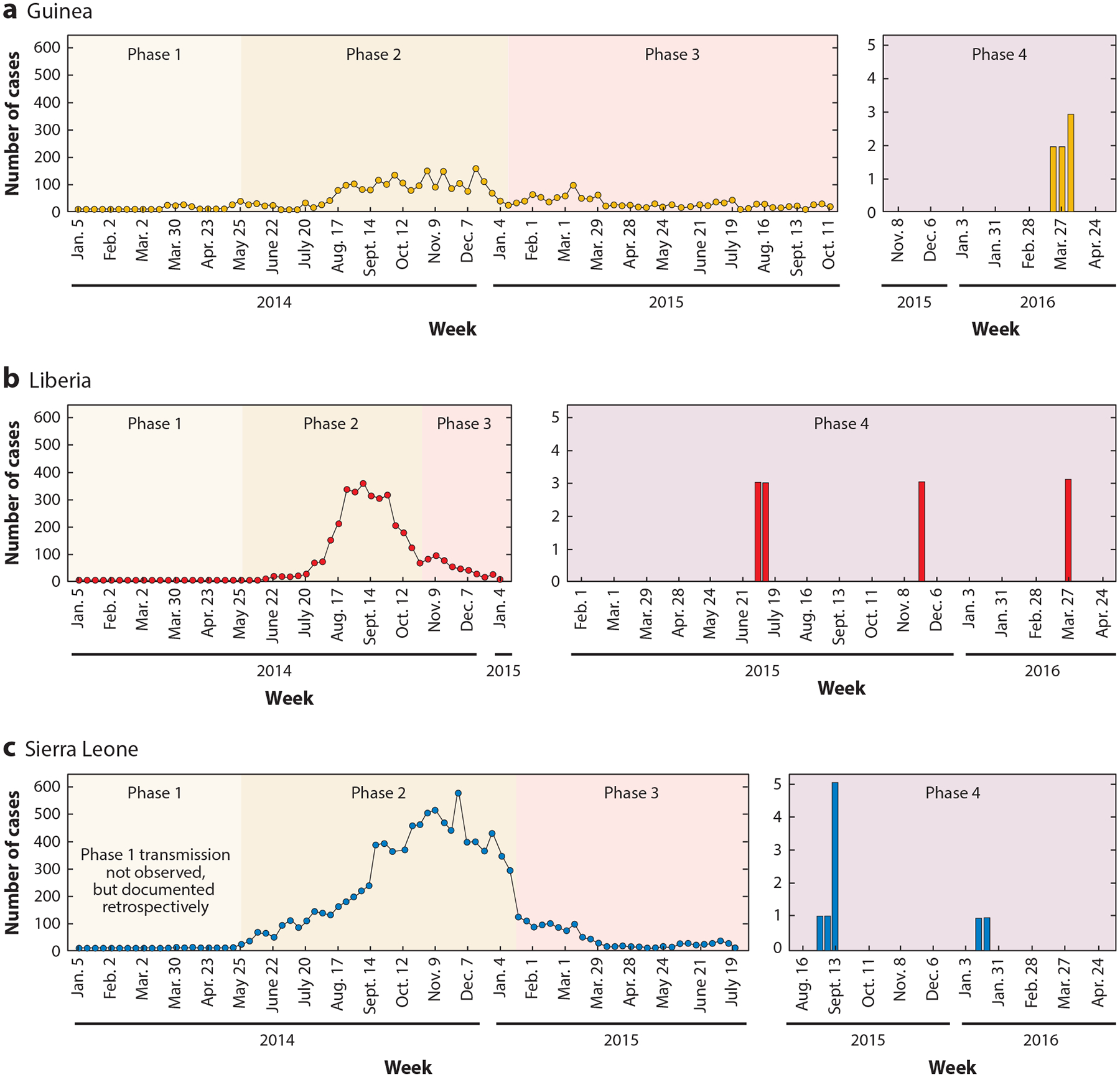
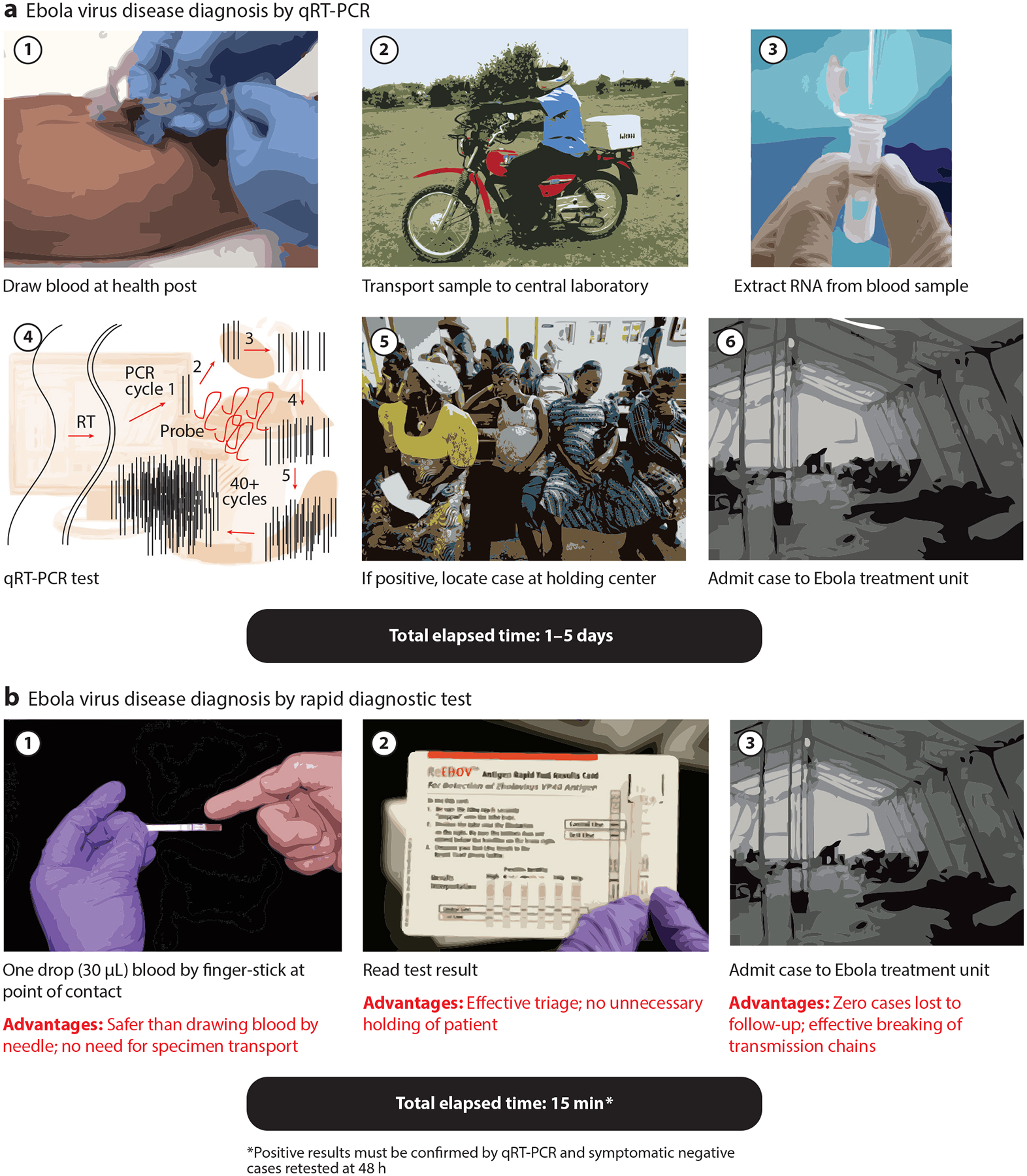
The 2013-16 West African Ebola outbreak is the largest, most geographically dispersed, and deadliest on record, with 28,616 suspected cases and 11,310 deaths recorded to date in Guinea, Liberia, and Sierra Leone. We provide a review of the epidemiology and management of the 2013-16 Ebola outbreak in West Africa aimed at stimulating reflection on lessons learned that may improve the response to the next international health crisis caused by a pathogen that emerges in a region of the world with a severely limited health care infrastructure. Surveillance efforts employing rapid and effective point-of-care diagnostics designed for environments that lack advanced laboratory infrastructure will greatly aid in early detection and containment efforts during future outbreaks. Introduction of effective therapeutics and vaccines against Ebola into the public health system and the biodefense armamentarium is of the highest priority if future outbreaks are to be adequately managed and contained in a timely manner.
Keywords: Ebola virus; epidemiology; filoviruses; outbreak management; point-of-care testing; viral diagnostics; viral genetics; viral therapeutics; viral vaccines.
Figures
References
LITERATURE CITED
-
- Amblard J, Obiang P, Edzang S, Prehaud C, Bouloy M, Guenno BLE. 1997. Identification of the Ebola virus in Gabon in 1994. Lancet 349:181–82 - PubMed
-
- Georges AJ, Leroy EM, Renaut AA, Benissan CT, Nabias RJ, et al. 1999. Ebola hemorrhagic fever outbreaks in Gabon, 1994–1997: epidemiologic and health control issues. J. Infect. Dis 179:S65–75 - PubMed
RELATED RESOURCES
-
- Sterk E, ed. 2008. Filovirus haemorrhagic fever guideline. L003HEFG03E, Médecins Sans Frontières, Geneva, Switz: http://www.medbox.org/ebola-guidelines/filovirus-haemorrhagic-fever-guid...
-
- US FDA. 2014. Emergency Use Authorization: Ebola virus EUA information. US FDA, Silver Spring, Md: Updated July 7, 2016. http://www.fda.gov/EmergencyPreparedness/Counterterrorism/MedicalCounter...
-
- WHO. 2014. Case definition recommendations for Ebola or Marburg virus diseases. WHO/EVD/CaseDef/14.1, WHO, Geneva, Switz: http://www.who.int/csr/resources/publications/ebola/case-definition/en/
-
- WHO. 2014. Ebola publications: vaccines, research and development. WHO, Geneva, Switz: Updated April 2016. http://www.who.int/csr/resources/publications/ebola/vaccines/en/
-
- WHO. 2015. Interim guidance on the use of rapid Ebola antigen detection tests. WHO/EVD/HIS/EMP/15.1, WHO, Geneva, Switz: http://www.who.int/csr/resources/publications/ebola/ebola-antigen-detect...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
