

Bariatric Surgery and Long-term Durability of Weight Loss
- PMID: 27579793
- PMCID: PMC5112115
- DOI: 10.1001/jamasurg.2016.2317
Bariatric Surgery and Long-term Durability of Weight Loss
Abstract
Importance: Bariatric surgery induces significant weight loss for severely obese patients, but there is limited evidence of the durability of weight loss compared with nonsurgical matches and across bariatric procedures.
Objectives: To examine 10-year weight change in a large, multisite, clinical cohort of veterans who underwent Roux-en-Y gastric bypass (RYGB) compared with nonsurgical matches and the 4-year weight change in veterans who underwent RYGB, adjustable gastric banding (AGB), or sleeve gastrectomy (SG).
Design, setting, and participants: In this cohort study, differences in weight change up to 10 years after surgery were estimated in retrospective cohorts of 1787 veterans who underwent RYGB from January 1, 2000, through September 30, 2011 (573 of 700 eligible [81.9%] with 10-year follow-up), and 5305 nonsurgical matches (1274 of 1889 eligible [67.4%] with 10-year follow-up) in mixed-effects models. Differences in weight change up to 4 years were compared among veterans undergoing RYGB (n = 1785), SG (n = 379), and AGB (n = 246). Data analysis was performed from September 9, 2014, to February 12, 2016.
Exposures: Bariatric surgical procedures and usual care.
Main outcomes and measures: Weight change up to 10 years after surgery through December 31, 2014.
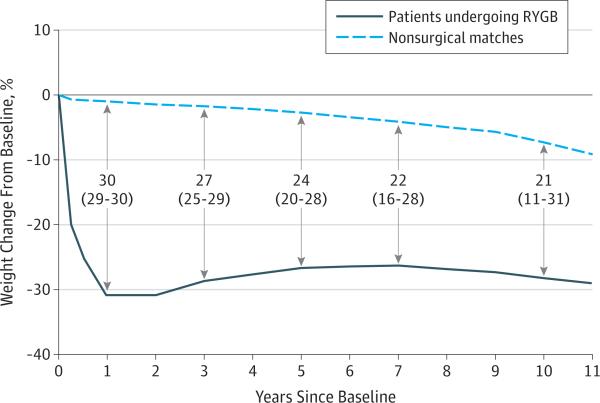
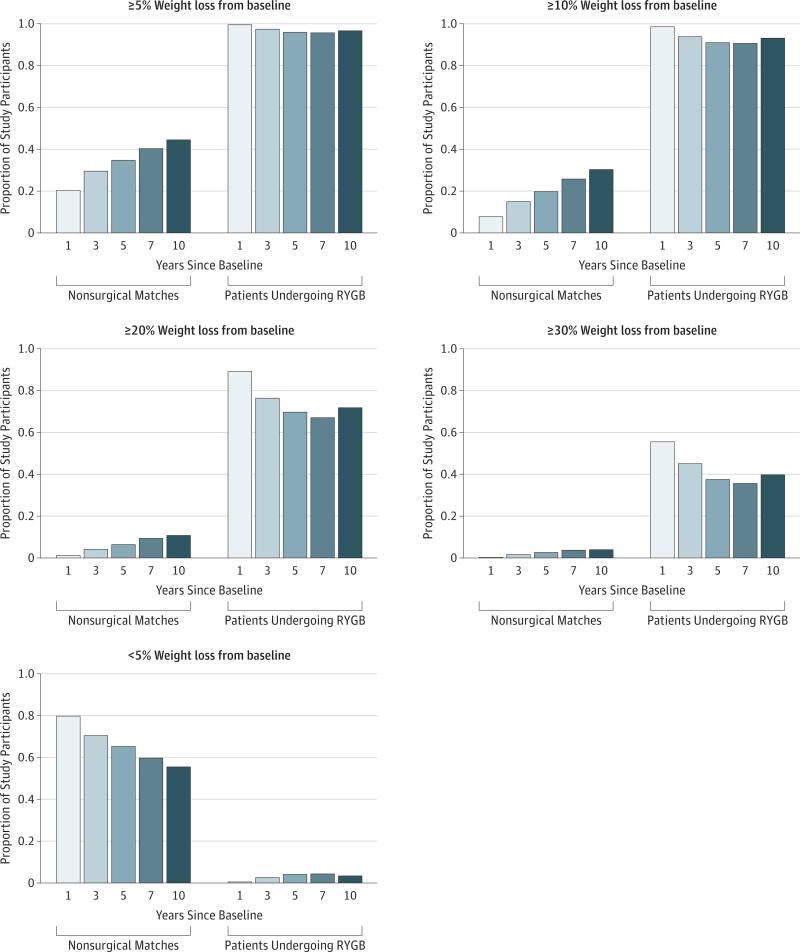
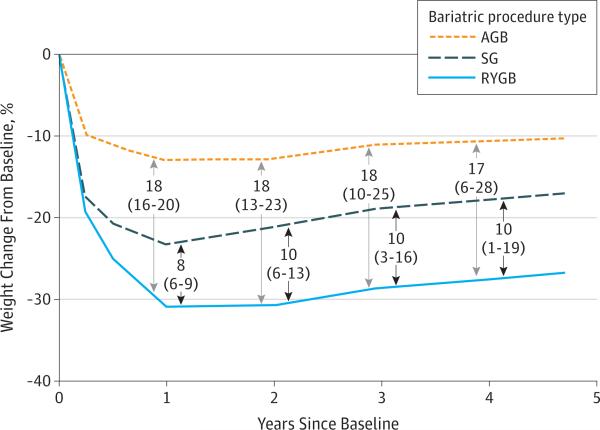
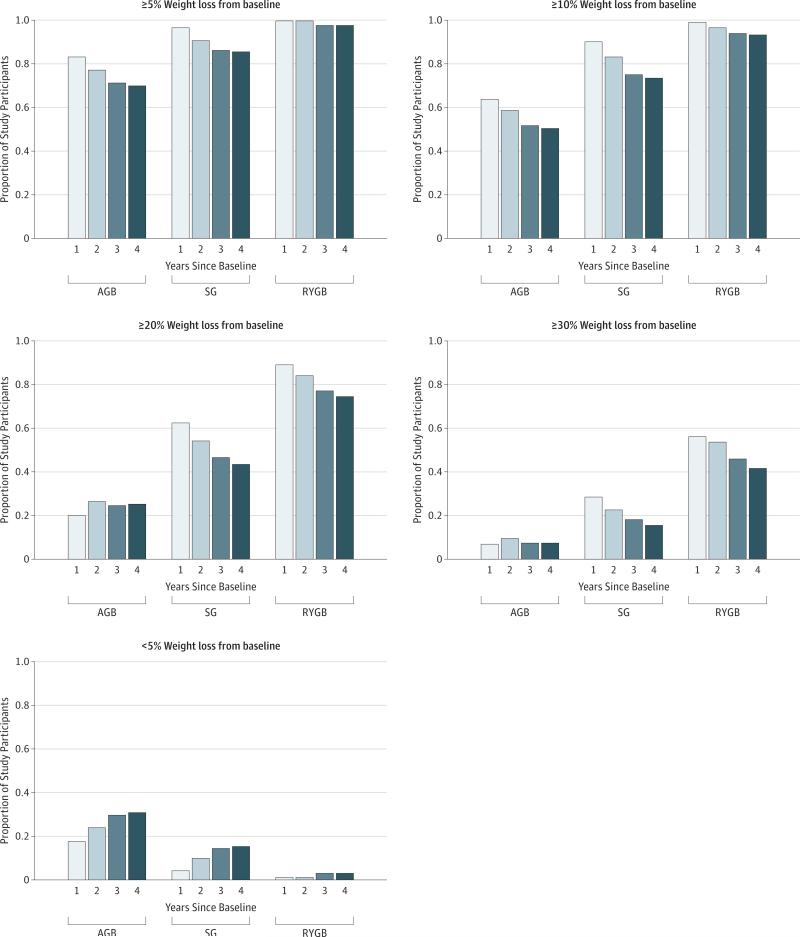
Results: The 1787 patients undergoing RYGB had a mean (SD) age of 52.1 (8.5) years and 5305 nonsurgical matches had a mean (SD) age of 52.2 (8.4) years. Patients undergoing RYGB and nonsurgical matches had a mean body mass index of 47.7 and 47.1, respectively, and were predominantly male (1306 [73.1%] and 3911 [73.7%], respectively). Patients undergoing RYGB lost 21% (95% CI, 11%-31%) more of their baseline weight at 10 years than nonsurgical matches. A total of 405 of 564 patients undergoing RYGB (71.8%) had more than 20% estimated weight loss, and 224 of 564 (39.7%) had more than 30% estimated weight loss at 10 years compared with 134 of 1247 (10.8%) and 48 of 1247 (3.9%), respectively, of nonsurgical matches. Only 19 of 564 patients undergoing RYGB (3.4%) regained weight back to within an estimated 5% of their baseline weight by 10 years. At 4 years, patients undergoing RYGB lost 27.5% (95% CI, 23.8%-31.2%) of their baseline weight, patients undergoing AGB lost 10.6% (95% CI, 0.6%-20.6%), and patients undergoing SG lost 17.8% (95% CI, 9.7%-25.9%). Patients undergoing RYGB lost 16.9% (95% CI, 6.2%-27.6%) more of their baseline weight than patients undergoing AGB and 9.7% (95% CI, 0.8%-18.6%) more than patients undergoing SG.
Conclusions and relevance: Patients in the Veterans Administration health care system lost substantially more weight than nonsurgical matches and sustained most of this weight loss in the long term. Roux-en-Y gastric bypass induced significantly greater weight loss among veterans than SG or AGB at 4 years. These results provide further evidence of the beneficial association between surgery and long-term weight loss that has been demonstrated in shorter-term studies of younger, predominantly female populations.
Figures
Comment in
-
Myths Surrounding Bariatric Surgery.JAMA Surg. 2016 Nov 1;151(11):1055. doi: 10.1001/jamasurg.2016.2301. JAMA Surg. 2016. PMID: 27579624 No abstract available.
References
-
- Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724–1737. - PubMed
-
- Picot J, Jones J, Colquitt JL, et al. The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation. Health Technol Assess. 2009;13(41):1–190, 215-357, iii-iv. - PubMed
-
- Trastulli S, Desiderio J, Guarino S, et al. Laparoscopic sleeve gastrectomy compared with other bariatric surgical procedures: a systematic review of randomized trials. Surg Obes Relat Dis. 2013;9(5):816–829. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
