

Impact of a Value-based Formulary on Medication Utilization, Health Services Utilization, and Expenditures
- PMID: 27579915
- PMCID: PMC5233590
- DOI: 10.1097/MLR.0000000000000630
Impact of a Value-based Formulary on Medication Utilization, Health Services Utilization, and Expenditures
Abstract
Background: Value-based benefit design has been suggested as an effective approach to managing the high cost of pharmaceuticals in health insurance markets. Premera Blue Cross, a large regional health plan, implemented a value-based formulary (VBF) for pharmaceuticals in 2010 that explicitly used cost-effectiveness analysis (CEA) to inform medication copayments.
Objective of the study: The objective of the study was to determine the impact of the VBF.
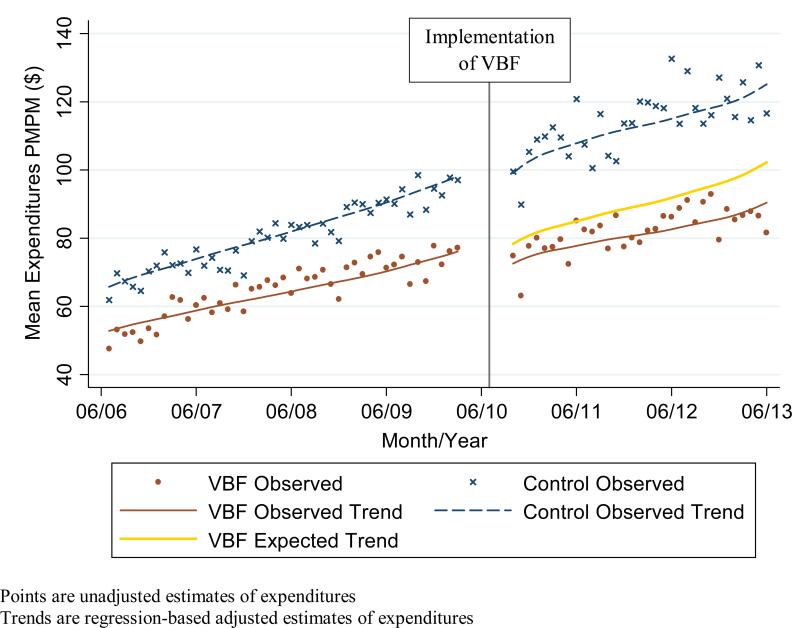
Design: Interrupted time series of employer-sponsored plans from 2006 to 2013.
Subjects: Intervention group: 5235 beneficiaries exposed to the VBF.
Control group: 11,171 beneficiaries in plans without any changes in pharmacy benefits.
Intervention: The VBF-assigned medications with lower value (estimated by CEA) to higher copayment tiers and assigned medications with higher value to lower copayment tiers.
Measures: Primary outcome was medication expenditures from member, health plan, and member plus health plan perspectives. Secondary outcomes were medication utilization, emergency department visits, hospitalizations, office visits, and nonmedication expenditures.
Results: In the intervention group after VBF implementation, member medication expenditures increased by $2 per member per month (PMPM) [95% confidence interval (CI), $1-$3] or 9%, whereas health plan medication expenditures decreased by $10 PMPM (CI, $18-$2) or 16%, resulting in a net decrease of $8 PMPM (CI, $15-$2) or 10%, which translates to a net savings of $1.1 million. Utilization of medications moved into lower copayment tiers increased by 1.95 days' supply (CI, 1.29-2.62) or 17%. Total medication utilization, health services utilization, and nonmedication expenditures did not change.
Conclusions: Cost-sharing informed by CEA reduced overall medication expenditures without negatively impacting medication utilization, health services utilization, or nonmedication expenditures.
Figures
References
-
- Kaiser Family Foundation and Health Research and Educational Trust [4/22/14];The Uninsured: A Primer - Key Facts about Health Insurance on the Eve of Coverage Expansions. 2013 http://kff.org/report-section/the-uninsured-a-primer-2013-introduction/.
-
- Kaiser Family Foundation and Health Research and Educational Trust . 2014 employer health benefits survey. KFF; Menlo Park, CA: 2014. [4/5/15]. http://files.kff.org/attachment/2014-employer-health-benefits-survey-ful....
-
- Martin AB, Hartman M, Benson J, Catlin A, National Health Expenditure Accounts T. National Health Spending In 2014: Faster Growth Driven By Coverage Expansion And Prescription Drug Spending. Health affairs. 2016 Jan 1;35(1):150–160. - PubMed
-
- Fendrick AM, Smith DG, Chernew ME, Shah SN. A benefit-based copay for prescription drugs: patient contribution based on total benefits, not drug acquisition cost. The American journal of managed care. 2001 Sep;7(9):861–867. - PubMed
-
- Fendrick AM, Chernew ME. Value-based insurance design: a “clinically sensitive” approach to preserve quality of care and contain costs. The American journal of managed care. 2006 Jan;12(1):18–20. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
