

Potential Strategies to Address the Major Clinical Barriers Facing Stem Cell Regenerative Therapy for Cardiovascular Disease: A Review
- PMID: 27579998
- PMCID: PMC5378463
- DOI: 10.1001/jamacardio.2016.2750
Potential Strategies to Address the Major Clinical Barriers Facing Stem Cell Regenerative Therapy for Cardiovascular Disease: A Review
Abstract
Importance: Although progress continues to be made in the field of stem cell regenerative medicine for the treatment of cardiovascular disease, significant barriers to clinical implementation still exist.
Objectives: To summarize the current barriers to the clinical implementation of stem cell therapy in patients with cardiovascular disease and to discuss potential strategies to overcome them.
Evidence review: Information for this review was obtained through a search of PubMed and the Cochrane database for English-language studies published between January 1, 2000, and July 25, 2016. Ten randomized clinical trials and 8 systematic reviews were included.
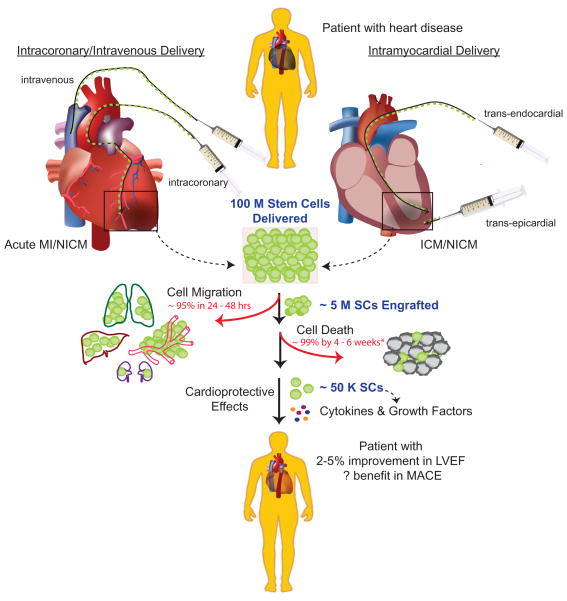
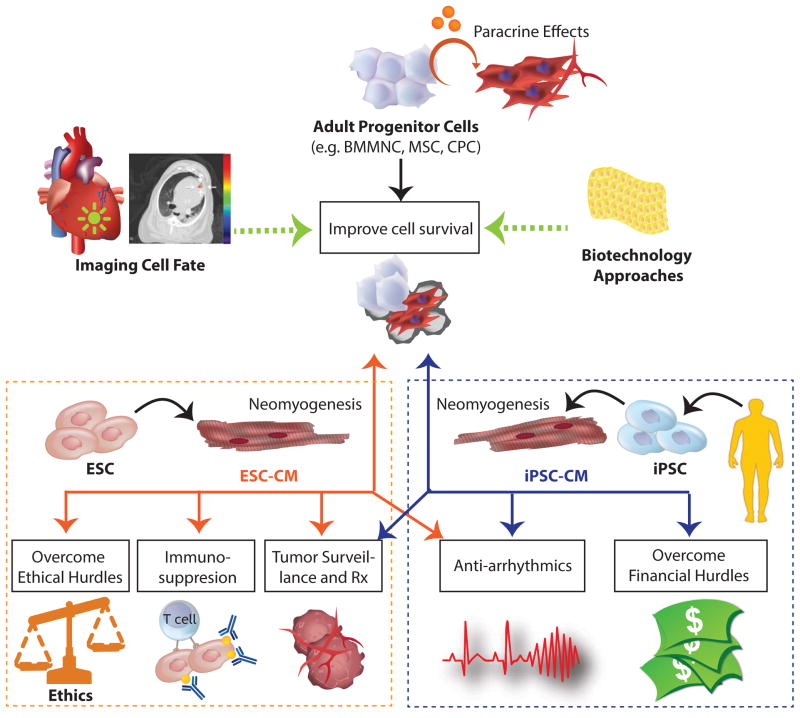
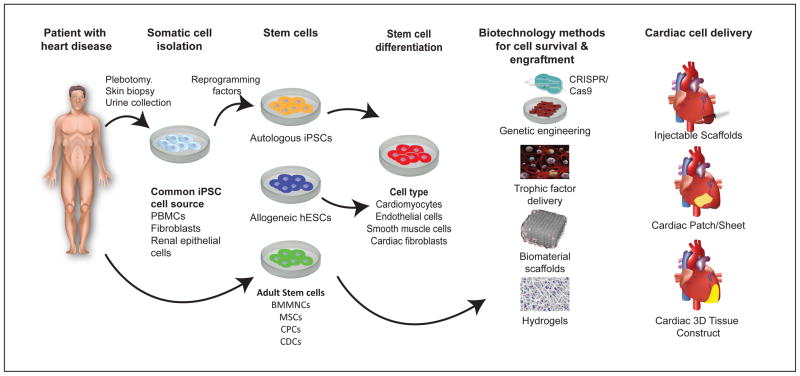
Findings: One of the major clinical barriers facing the routine implementation of stem cell therapy in patients with cardiovascular disease is the limited and inconsistent benefit observed thus far. Reasons for this finding are unclear but may be owing to poor cell retention and survival, as suggested by numerous preclinical studies and a small number of human studies incorporating imaging to determine cell fate. Additional studies in humans using imaging to determine cell fate are needed to understand how these factors contribute to the limited efficacy of stem cell therapy. Treatment strategies to address poor cell retention and survival are under investigation and include the following: coadministration of immunosuppressive and prosurvival agents, delivery of cardioprotective factors packaged in exosomes rather than the cells themselves, and use of tissue-engineering strategies to provide structural support for cells. If larger grafts are achieved using these strategies, it will be imperative to carefully monitor for the potential risks of tumorigenicity, immunogenicity, and arrhythmogenicity.
Conclusions and relevance: Despite important achievements to date, stem cell therapy is not yet ready for routine clinical implementation. Significant research is still needed to address the clinical barriers outlined herein before the next wave of large clinical trials is under way.
Figures
References
-
- Pavo N, Charwat S, Nyolczas N, et al. Cell therapy for human ischemic heart diseases: critical review and summary of the clinical experiences. J Mol Cell Cardiol. 2014;75:12–24. - PubMed
-
- Wollert KC, Drexler H. Cell therapy for the treatment of coronary heart disease: a critical appraisal. Nature Reviews. Cardiology. 2010;7:204–215. - PubMed
-
- Fisher Sheila A, Brunskill Susan J, Doree C, Mathur A, Taggart David P, Martin-Rendon E. Stem cell therapy for chronic ischaemic heart disease and congestive heart failure. Cochrane Database of Systematic Reviews. 2014 - PubMed
-
- Martin-Rendon E, Brunskill SJ, Hyde CJ, Stanworth SJ, Mathur A, Watt SM. Autologous bone marrow stem cells to treat acute myocardial infarction: a systematic review. Eur Heart J. 2008;29(15):1807–1818. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
