

What MRI Findings Predict Failure 10 Years After Surgery for Femoroacetabular Impingement?
- PMID: 27580735
- PMCID: PMC5339116
- DOI: 10.1007/s11999-016-5040-8
What MRI Findings Predict Failure 10 Years After Surgery for Femoroacetabular Impingement?
Erratum in
-
Erratum to: What MRI Findings Predict Failure 10 Years After Surgery for Femoroacetabular Impingement?Clin Orthop Relat Res. 2017 Apr;475(4):1278. doi: 10.1007/s11999-016-5075-x. Clin Orthop Relat Res. 2017. PMID: 27620802 Free PMC article. No abstract available.
Abstract
Background: Magnetic resonance arthrogram (MRA) with radial cuts is presently the best available preoperative imaging study to evaluate chondrolabral lesions in the setting of femoroacetabular impingement (FAI). Existing followup studies for surgical treatment of FAI have evaluated predictors of treatment failure based on preoperative clinical examination, intraoperative findings, and conventional radiography. However, to our knowledge, no study has examined whether any preoperative findings on MRA images might be associated with failure of surgical treatment of FAI in the long term.
Questions/purposes: The purposes of this study were (1) to identify the preoperative MRA findings that are associated with conversion to THA, any progression of osteoarthritis, and/or a Harris hip score of < 80 points after acetabuloplasty and/or osteochondroplasty of the femoral head-neck junction through a surgical hip dislocation (SHD) for FAI at a minimum 10-year followup; and (2) identify the age of patients with symptomatic FAI when these secondary degenerative findings were detected on preoperative radial MRAs.
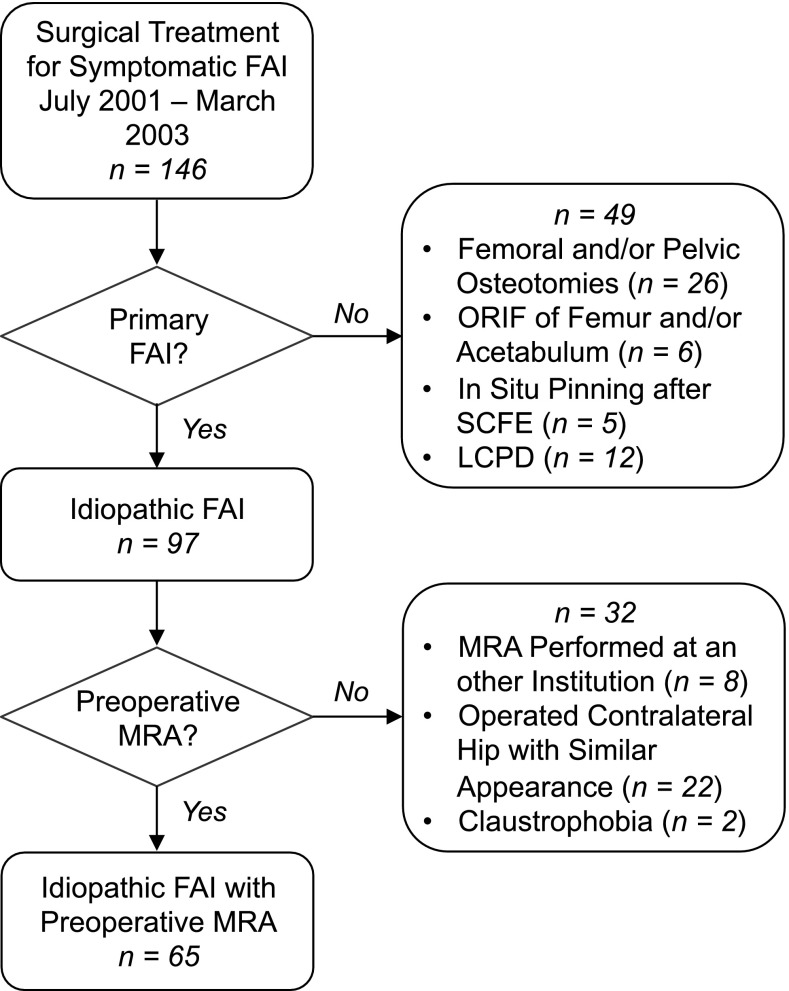
Methods: We retrospectively studied 121 patients (146 hips) who underwent acetabuloplasty and/or osteochondroplasty of the femoral head-neck junction through SHD for symptomatic anterior FAI between July 2001 and March 2003. We excluded 35 patients (37 hips) with secondary FAI after previous surgery and 11 patients (12 hips) with Legg-Calvé-Perthes disease. All patients underwent preoperative MRA to further specify chondrolabral lesions except in 19 patients (32 hips) including 17 patients (20 hips) who presented with an MRI from an external institution taken with a different protocol, 10 patients with no preoperative MRA because the patients had already been operated on the contralateral side with a similar appearance, and two patients (two hips) refused MRA because of claustrophobia. This resulted in 56 patients (65 hips) with idiopathic FAI and a preoperative MRA. Of those, three patients (three hips) did not have minimal 10-year followup (one patient died; two hips with followup between 5 and 6 years). The remaining patients were evaluated clinically and radiographically at a mean followup of 11 years (range, 10-13 years). Thirteen pathologic radiographic findings on the preoperative MRA were evaluated for an association with the following endpoints using Cox regression analysis: conversion to THA, radiographic evidence of any progression of osteoarthritis, and/or a Harris hip score of < 80. The age of the patient when each degenerative pattern was found on the preoperative MRA was recorded.
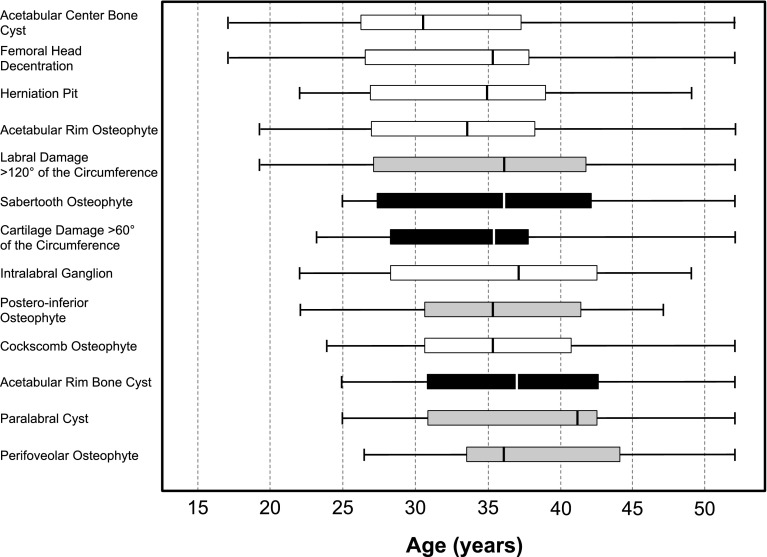
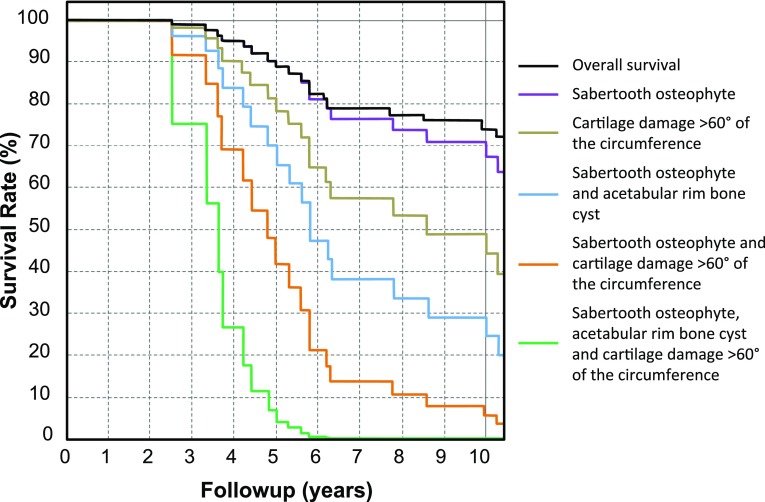
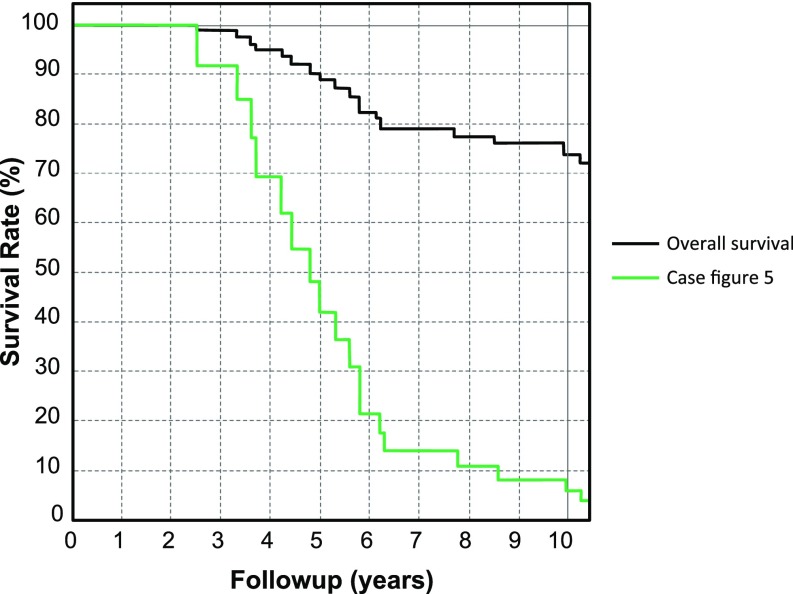
Results: The following MRI findings were associated with one or more of our predefined failure endpoints: cartilage damage exceeding 60° of the circumference had a hazard ratio (HR) of 4.6 (95% confidence interval [CI], 3.6-5.6; p = 0.003) compared with a damage of less than 60°, presence of an acetabular rim cyst had a HR of 4.1 (95% CI, 3.1-5.2; p = 0.008) compared with hips without these cysts, and presence of a sabertooth osteophyte had a HR of 3.2 (95% CI, 2.3-4.2; p = 0.013) compared with hips without a sabertooth osteophyte. The degenerative pattern associated with the youngest patient age when detected on preoperative MRA was the sabertooth osteophyte (lower quartile 27 years) followed by cartilage damage exceeding 60° of the circumference (28 years) and the presence of an acetabular rim bone cyst (31 years).
Conclusions: Preoperative MRAs with radial cuts reveal important findings that may be associated with future failure of surgical treatment for FAI. Most of these factors are not visible on conventional radiographs or standard hip MRIs. Preoperative MRA evaluation is therefore strongly recommended on a routine basis for patients undergoing these procedures. Findings associated with conversion to arthroplasty, radiographic evidence of any progression of osteoarthritis, and/or a Harris hip score of < 80 points should be incorporated into the decision-making process in patients being evaluated for joint-preserving hip surgery.
Level of evidence: Level III, therapeutic study.
Figures

Comment in
-
CORR Insights®: What MRI Findings Predict Failure 10 Years After Surgery for Femoroacetabular Impingement?Clin Orthop Relat Res. 2017 Apr;475(4):1208-1211. doi: 10.1007/s11999-016-5085-8. Epub 2016 Sep 20. Clin Orthop Relat Res. 2017. PMID: 27650991 Free PMC article. No abstract available.
Similar articles
-
What Are the Risk Factors for Revision Surgery After Hip Arthroscopy for Femoroacetabular Impingement at 7-year Followup?Clin Orthop Relat Res. 2017 Apr;475(4):1169-1177. doi: 10.1007/s11999-016-5115-6. Clin Orthop Relat Res. 2017. PMID: 27718121 Free PMC article.
-
One-third of Hips After Periacetabular Osteotomy Survive 30 Years With Good Clinical Results, No Progression of Arthritis, or Conversion to THA.Clin Orthop Relat Res. 2017 Apr;475(4):1154-1168. doi: 10.1007/s11999-016-5169-5. Clin Orthop Relat Res. 2017. PMID: 27905061 Free PMC article.
-
How Does the dGEMRIC Index Change After Surgical Treatment for FAI? A Prospective Controlled Study: Preliminary Results.Clin Orthop Relat Res. 2017 Apr;475(4):1080-1099. doi: 10.1007/s11999-016-5098-3. Clin Orthop Relat Res. 2017. PMID: 27709422 Free PMC article.
-
Beyond the Scope Open Treatment of Femoroacetabular Impingement.Bull Hosp Jt Dis (2013). 2018 Mar;76(1):47-54. Bull Hosp Jt Dis (2013). 2018. PMID: 29537957 Review.
-
What is the evidence supporting the prevention of osteoarthritis and improved femoral coverage after shelf procedure for Legg-Calvé-Perthes disease?Clin Orthop Relat Res. 2012 Sep;470(9):2421-30. doi: 10.1007/s11999-011-2220-4. Clin Orthop Relat Res. 2012. PMID: 22194022 Free PMC article.
Cited by
-
Advances in FAI Imaging: a Focused Review.Curr Rev Musculoskelet Med. 2020 Oct;13(5):622-640. doi: 10.1007/s12178-020-09663-7. Curr Rev Musculoskelet Med. 2020. PMID: 32845416 Free PMC article. Review.
-
Biochemical MRI With dGEMRIC Corresponds to 3D-CT Based Impingement Location for Detection of Acetabular Cartilage Damage in FAI Patients.Orthop J Sports Med. 2021 Mar 19;9(3):2325967120988175. doi: 10.1177/2325967120988175. eCollection 2021 Mar. Orthop J Sports Med. 2021. PMID: 33816640 Free PMC article.
-
Automated quantification of cartilage quality for hip treatment decision support.Int J Comput Assist Radiol Surg. 2022 Nov;17(11):2011-2021. doi: 10.1007/s11548-022-02714-z. Epub 2022 Aug 17. Int J Comput Assist Radiol Surg. 2022. PMID: 35976596 Free PMC article.
-
Automatic MRI-based Three-dimensional Models of Hip Cartilage Provide Improved Morphologic and Biochemical Analysis.Clin Orthop Relat Res. 2019 May;477(5):1036-1052. doi: 10.1097/CORR.0000000000000755. Clin Orthop Relat Res. 2019. PMID: 30998632 Free PMC article.
-
Ischiofemoral impingement in joint preserving hip surgery: prevalence and imaging predictors.Insights Imaging. 2025 Apr 4;16(1):78. doi: 10.1186/s13244-025-01946-2. Insights Imaging. 2025. PMID: 40186048 Free PMC article.
References
-
- Altman DG. Practical Statistics for Medical Research. London, UK: Chapman & Hall/CRC; 1991.
-
- d’Aubigné RM, Postel M. Functional results of hip arthroplasty with acrylic prosthesis. J Bone Joint Surg Am. 1954;36:451–475. - PubMed
-
- Beaulé PE, Le Duff MJ, Zaragoza E. Quality of life following femoral head-neck osteochondroplasty for femoroacetabular impingement. J Bone Joint Surg Am. 2007;89:773–779. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
