

Dysfunctional breathing: a review of the literature and proposal for classification
- PMID: 27581828
- PMCID: PMC9487208
- DOI: 10.1183/16000617.0088-2015
Dysfunctional breathing: a review of the literature and proposal for classification
Abstract
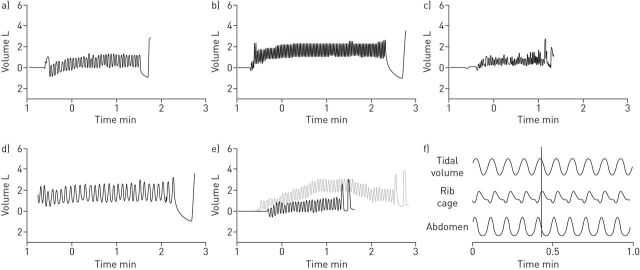
Dysfunctional breathing is a term describing breathing disorders where chronic changes in breathing pattern result in dyspnoea and other symptoms in the absence or in excess of the magnitude of physiological respiratory or cardiac disease. We reviewed the literature and propose a classification system for the common dysfunctional breathing patterns described. The literature was searched using the terms: dysfunctional breathing, hyperventilation, Nijmegen questionnaire and thoraco-abdominal asynchrony. We have summarised the presentation, assessment and treatment of dysfunctional breathing, and propose that the following system be used for classification. 1) Hyperventilation syndrome: associated with symptoms both related to respiratory alkalosis and independent of hypocapnia. 2) Periodic deep sighing: frequent sighing with an irregular breathing pattern. 3) Thoracic dominant breathing: can often manifest in somatic disease, if occurring without disease it may be considered dysfunctional and results in dyspnoea. 4) Forced abdominal expiration: these patients utilise inappropriate and excessive abdominal muscle contraction to aid expiration. 5) Thoraco-abdominal asynchrony: where there is delay between rib cage and abdominal contraction resulting in ineffective breathing mechanics.This review highlights the common abnormalities, current diagnostic methods and therapeutic implications in dysfunctional breathing. Future work should aim to further investigate the prevalence, clinical associations and treatment of these presentations.
Copyright ©ERS 2016.
Conflict of interest statement
Conflict of interest: None declared.
Figures
References
-
- Folgering H. The pathophysiology of hyperventilation syndrome. Monaldi Arch Chest Dis 1999; 54: 365–372. - PubMed
-
- Gardner WN. The pathophysiology of hyperventilation disorders. Chest 1996; 109: 516–534. - PubMed
-
- Jack S, Rossiter HB, Pearson MG, et al. . Ventilatory responses to inhaled carbon dioxide, hypoxia, and exercise in idiopathic hyperventilation. Am J Respir Crit Care Med 2004; 170: 118–125. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical