

The Costs of Fall-Related Injuries among Older Adults: Annual Per-Faller, Service Component, and Patient Out-of-Pocket Costs
- PMID: 27581952
- PMCID: PMC5583303
- DOI: 10.1111/1475-6773.12554
The Costs of Fall-Related Injuries among Older Adults: Annual Per-Faller, Service Component, and Patient Out-of-Pocket Costs
Abstract
Objective: To estimate expenditures for fall-related injuries (FRIs) among older Medicare beneficiaries.
Data sources: The 2007-2009 Medicare claims and 2008 Health and Retirement Study (HRS) data for 5,497 (228 FRI and 5,269 non-FRI) beneficiaries.
Study design: FRIs were indicated by inpatient/outpatient ICD-9 diagnostic codes for fractures, trauma, dislocations, and by e-codes. A pre-post comparison group design was used to estimate the differential change in pre-post expenditures for the FRI relative to the non-FRI cohort (FRI expenditures). Out-of-pocket (OOP) costs, service category total annual FRI-related Medicare expenditures, expenditures related to the type of initial FRI treatment (inpatient, ED, outpatient), and the risk of persistently high expenditures (4th quartile for each post-FRI quarter) were estimated.
Principal findings: Estimated FRI expenditures were $9,389 (95 percent CI: $5,969-$12,808). Inpatient, physician/outpatient, skilled nursing facility, and home health comprised 31, 18, 39, and 12 percent of the total. OOP costs were $1,363.0 (95 percent CI: $889-$1,837). Expenditures for FRIs initially treated in inpatient/ED/outpatient settings were $21,424/$6,142/$8,622. The FRI cohort had a 64 percent increased risk of persistently high expenditures. Total Medicare expenditures were $13 billion (95 percent CI: $9-$18 billion).
Conclusions: FRIs are associated with substantial, persistent Medicare expenditures. Cost-effectiveness of multifactorial falls prevention programs should be assessed using these expenditure estimates.
Keywords: Medicare; direct medical expenditures; elderly; fall-related injuries; falls.
© Health Research and Educational Trust.
Figures
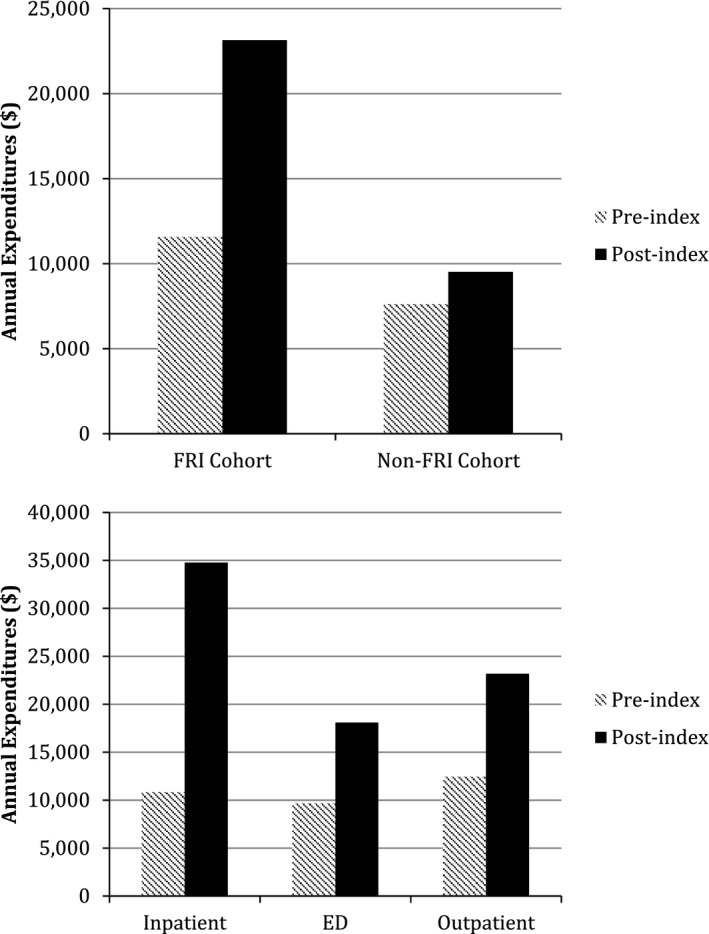
Notes. Unadjusted expenditures for the 5,497 individuals in the analytic sample of the main model (using the case‐crossover with comparison group study design). Injuries are those that were identified as index FRIs in the analysis.
References
-
- Annest, J. L. , Fingerhut L. A., Gallagher S. S., Grossman D. C., Hedegaard H., Johnson R. L., Kohn M., Pickett D., Thomas K. E., and Trent R. B.. 2008. “Strategies to Improve External Cause‐of‐Injury Coding in State‐Based Hospital Discharge and Emergency Department Data Systems: Recommendations of the CDC Workgroup for Improvement of External Cause‐of‐Injury Coding.” MMWR—Recommendations and Reports 57 (RR‐1): 1–15. - PubMed
-
- Blank, W. A. , Freiberger E., Siegrist M., Landendoerfer P., Linde K., Schuster T., Pfeifer K., Schneider A., and Halle M.. 2011. “An Interdisciplinary Intervention to Prevent Falls in Community‐Dwelling Elderly Persons: Protocol of a Cluster‐Randomized Trial [PreFalls].” BMC Geriatrics 11: 7. - PMC - PubMed
-
- Boards of Trustees . 2011. “2011 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds.” The Boards of Trustees, Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds.
-
- Bohl, A. A. , Fishman P. A., Ciol M. A., Williams B., Logerfo J., and Phelan E. A.. 2010. “A Longitudinal Analysis of Total 3‐year Healthcare Costs for Older Adults Who Experience a Fall Requiring Medical Care.” Journal of the American Geriatrics Society 58 (5): 853–60. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
