

Impact of Pulmonary Hemodynamics and Ventricular Interdependence on Left Ventricular Diastolic Function in Children With Pulmonary Hypertension
- PMID: 27581953
- PMCID: PMC5012318
- DOI: 10.1161/CIRCIMAGING.116.004612
Impact of Pulmonary Hemodynamics and Ventricular Interdependence on Left Ventricular Diastolic Function in Children With Pulmonary Hypertension
Abstract
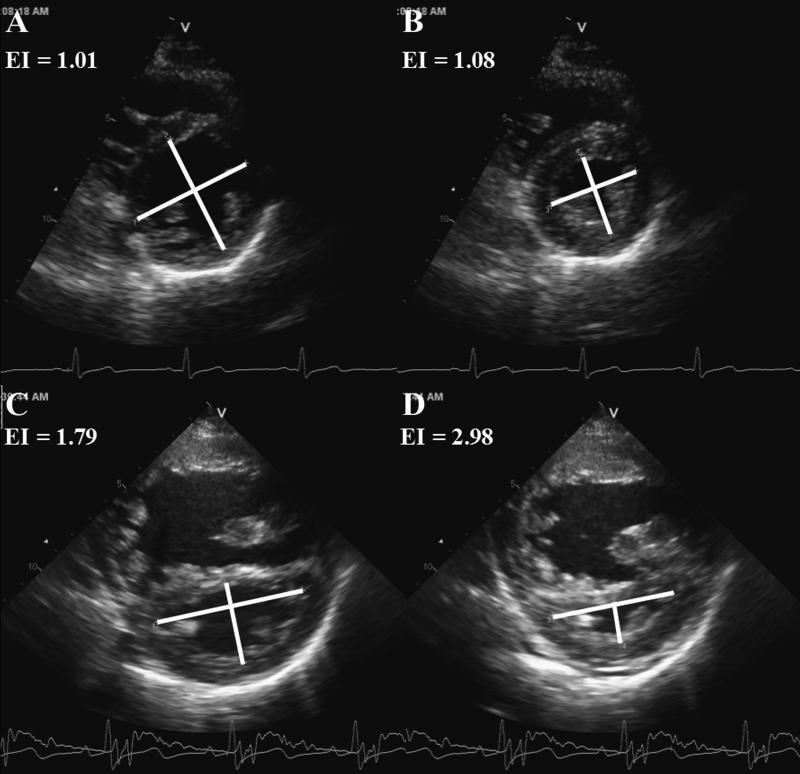
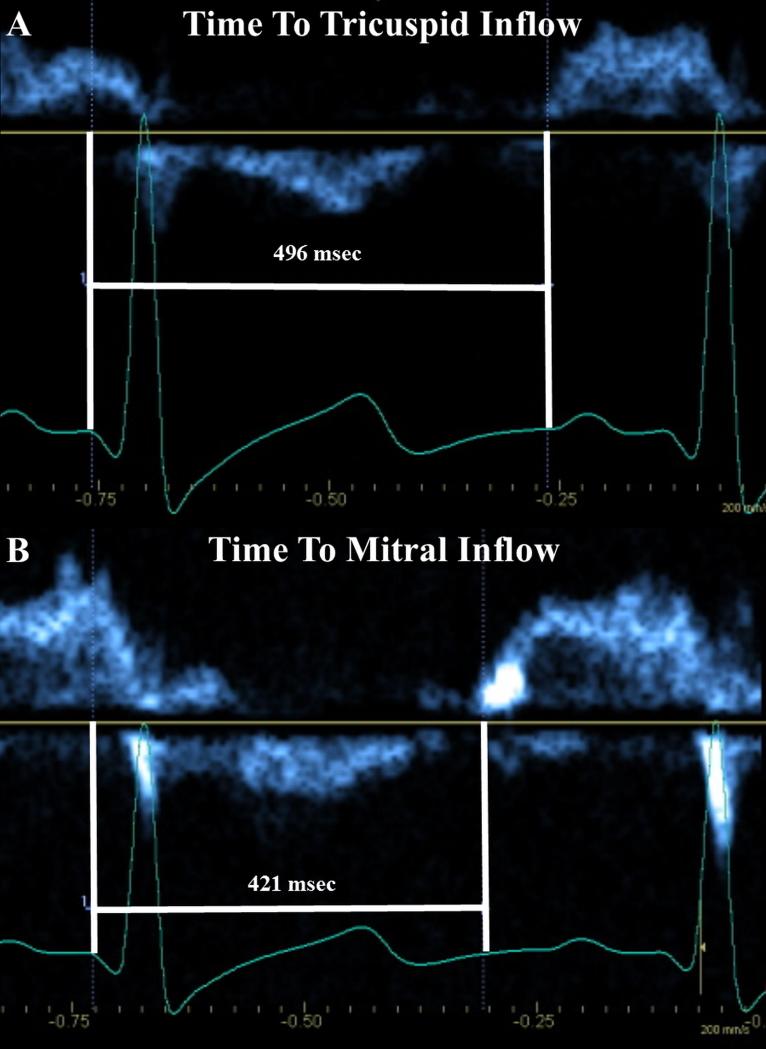
Background: Through ventricular interdependence, pulmonary hypertension (PH) induces left ventricular (LV) dysfunction. We hypothesized that pediatric PH patients have LV diastolic dysfunction, related to adverse pulmonary hemodynamics, leftward septal shift, and prolonged right ventricular systole.
Methods and results: Echocardiography was prospectively performed at 2 institutions in 54 pediatric PH patients during cardiac catheterization and in 54 matched controls. Diastolic LV measures including myocardial deformation were assessed by echocardiography. PH patients had evidence of LV diastolic dysfunction, most consistent with impaired LV relaxation, though some features of reduced ventricular compliance were present. PH patients demonstrated the following: reduced mitral E velocity and inflow duration, mitral E' and E'/A', septal E' and A', pulmonary vein S and D wave velocities, and LV basal global early diastolic circumferential strain rate and increased mitral E deceleration time, LV isovolumic relaxation time, mitral E/E', and pulmonary vein A wave duration. PH patients demonstrated leftward septal shift and prolonged right ventricular systole, both known to affect LV diastole. These changes were exacerbated in severe PH. There were no statistically significant differences in diastolic measures between patients with and without a shunt and minimal differences between patients with and without congenital heart disease. Multiple echocardiographic LV diastolic parameters demonstrated weak-to-moderate correlations with invasively determined PH severity, leftward septal shift, and prolonged right ventricular systole.
Conclusions: Pediatric PH patients exhibit LV diastolic dysfunction most consistent with impaired relaxation and reduced myocardial deformation, related to invasive hemodynamics, leftward septal shift, and prolonged right ventricular systole.
Keywords: cardiac catheterization; diastole; echocardiography; hypertension, pulmonary; pediatrics.
© 2016 American Heart Association, Inc.
Figures
Comment in
-
Left Ventricular Diastolic Dysfunction in Pediatric Pulmonary Hypertension.Circ Cardiovasc Imaging. 2016 Sep;9(9):e005527. doi: 10.1161/CIRCIMAGING.116.005527. Circ Cardiovasc Imaging. 2016. PMID: 27581954 No abstract available.
References
-
- D'Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Kernis JT, Levy PS, Pietra GG, Reid LM, Reeves JT, Rich S, Vreim CE, Williams GW, Wu M. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115:343–9. - PubMed
-
- Voelkel NF, Quaife RA, Leinwand LA, Barst RJ, McGoon MD, Meldrum DR, Dupuis J, Long CS, Rubin LJ, Smart FW, Suzuki YJ, Gladwin M, Denholm EM, Gail DB, National Heart L, Blood Institute Working Group on C Molecular Mechanisms of Right Heart F. Right ventricular function and failure: report of a National Heart, Lung, and Blood Institute working group on cellular and molecular mechanisms of right heart failure. Circulation. 2006;114:1883–91. - PubMed
-
- Chin KM, Kim NH, Rubin LJ. The right ventricle in pulmonary hypertension. Coron Artery Dis. 2005;16:13–8. - PubMed
-
- Bogaard HJ, Abe K, Vonk Noordegraaf A, Voelkel NF. The right ventricle under pressure: cellular and molecular mechanisms of right-heart failure in pulmonary hypertension. Chest. 2009;135:794–804. - PubMed
-
- Hardegree EL, Sachdev A, Fenstad ER, Villarraga HR, Frantz RP, McGoon MD, Oh JK, Ammash NM, Connolly HM, Eidem BW, Pellikka PA, Kane GC. Impaired left ventricular mechanics in pulmonary arterial hypertension: identification of a cohort at high risk. Circ Heart Fail. 2013;6:748–55. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
