

Efficacy, Safety, and Pharmacokinetics of a Novel Human Immune Globulin Subcutaneous, 20 % in Patients with Primary Immunodeficiency Diseases in North America
- PMID: 27582171
- PMCID: PMC5018260
- DOI: 10.1007/s10875-016-0327-9
Efficacy, Safety, and Pharmacokinetics of a Novel Human Immune Globulin Subcutaneous, 20 % in Patients with Primary Immunodeficiency Diseases in North America
Abstract
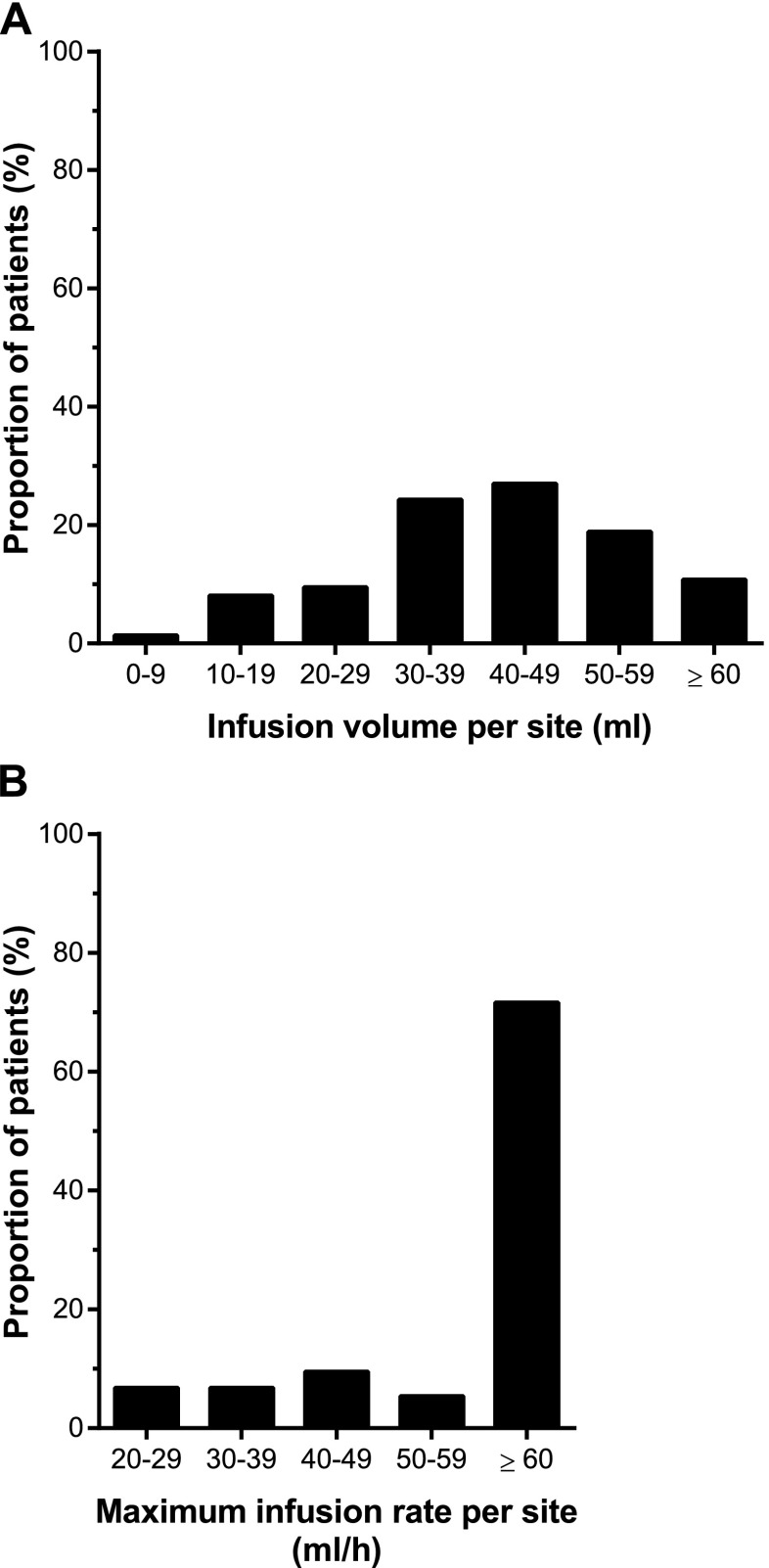
Patients with primary immunodeficiency disease (PIDD) typically require life-long intravenous (IV) or subcutaneous (SC) immunoglobulin (Ig) replacement therapy to prevent recurrent infections. The efficacy, safety, and pharmacokinetics of a highly concentrated (20 %) Ig preparation for SC administration (IGSC 20 %) were evaluated in a prospective trial in patients with PIDD. A total of 74 patients (aged 3-83 years) received 4327 IGSC 20 % infusions over a median of 380.5 days. The rate of validated serious bacterial infections was 0.012 event/patient-year (p < 0.0001 compared with the historical control), and the annualized rate of infection was 2.41 events/patient. Median IgG trough levels were >14.5 g/l. The median maximum infusion rate was 60 ml/h/site (range 4.4-180), resulting in a median infusion duration of 0.95 h. A volume ≥30 ml was infused per site in 74.8 % of IGSC 20 % infusions. Most (84.9 %) infusions were administered using ≤2 infusion sites; for 99.8 % of infusions, there was no need to interrupt/stop administration or reduce the infusion rate. No related serious adverse event (AE) occurred during IGSC 20 % treatment; related non-serious AEs occurred at a rate of 0.036 event/infusion. The incidence of related local AEs was 0.015 event/infusion and of related systemic AEs was 0.021 event/infusion; most were mild in severity, none severe. Increased infusion rates or volumes were not associated with higher AE rates. The investigated IGSC 20 % treatment was shown to be effective and safe, enabling higher infusion rates and volumes per site compared to conventional SC treatments, resulting in fewer infusion sites and shorter infusion durations.
Trial registration: ClinicalTrials.gov NCT01218438.
Keywords: 20 % immunoglobulin; Immunoglobulin replacement therapy; Pharmacokinetics; Primary immunodeficiency diseases; Subcutaneous administration.
Conflict of interest statement
Compliance with Ethical Standards This prospective, open-label clinical trial (registered on clinicaltrials.gov: NCT no. 01218438) was conducted in accordance with the Declaration of Helsinki and the international standards of Good Clinical Practice. Informed consent was obtained from each patient prior to undergoing any study procedures. Conflict of Interest DS, MS, SG, IH, KP, and AD worked as investigators on this Baxalta, now part of Shire-funded clinical study. DS, MS, and KP are on the Baxalta, now part of Shire advisory board and MS and KP have worked as speakers for Baxalta, now part of Shire. SG serves as an ad hoc advisor for Baxalta. CB, BM, HL, DG, and LY are full-time employees at Baxalta, now part of Shire. SF was a full-time employee of Baxalta, now part of Shire, at the time when this study was underway. BM, HL, and LY are shareholders of Baxalta, now part of Shire. Research involving human participants All procedures performed in the study were in accordance with the ethical standards of the institutional and /or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Figures

References
-
- Bruton OC. Agammaglobulinemia. Pediatrics. 1952;9:722–728. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
