

Review
doi: 10.1177/1758573214548934.
Epub 2014 Sep 4.
The clinical physiotherapy assessment of non-traumatic shoulder instability
Affiliations
- PMID: 27582958
- PMCID: PMC4935096
- DOI: 10.1177/1758573214548934
Item in Clipboard
Review
The clinical physiotherapy assessment of non-traumatic shoulder instability
Shoulder Elbow.
2015 Jan.
Abstract
Non-traumatic shoulder instability is frequently associated with chronic disabling pain, altered patterns of motion, dysfunctional muscle strategies and hyperlaxity. Identifying the relationship between potential aetiologies can be challenging. An expanded assessment may be useful to estimate the contribution of each component and offer a framework for targeted rehabilitation.
Keywords: Assessment; instability; non-traumatic; physiotherapy; shoulder.
Figures
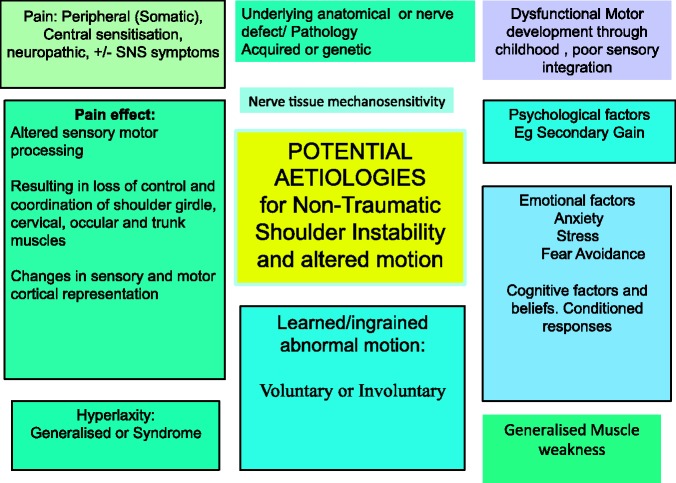
Potential aetiologies in nontraumatic (or atraumatic) shoulder instability.

Movement corrections, of trunk side flexion and upward scapula rotation through flexion, and correction of downward scapula rotation in ballet pose.
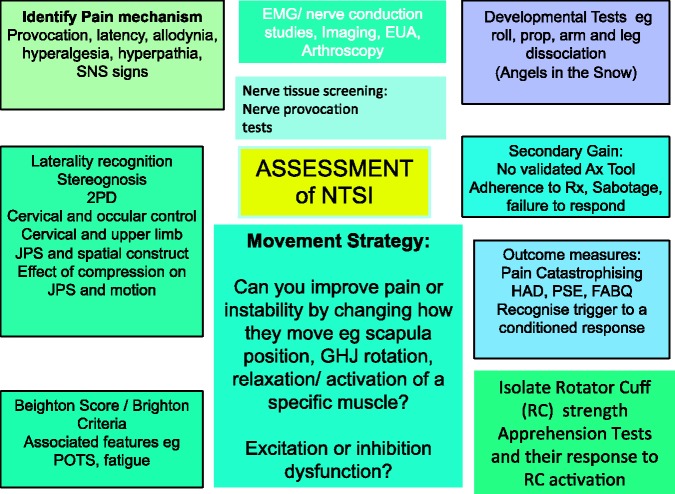
The assessment of potential aetiologies in non-traumatic (or atraumatic) shoulder instability.

Images showing how a downwardly rotated scapula (left) can be upwardly orientated into the correct position using the ‘Shrug’ (Watson et al. 2010).
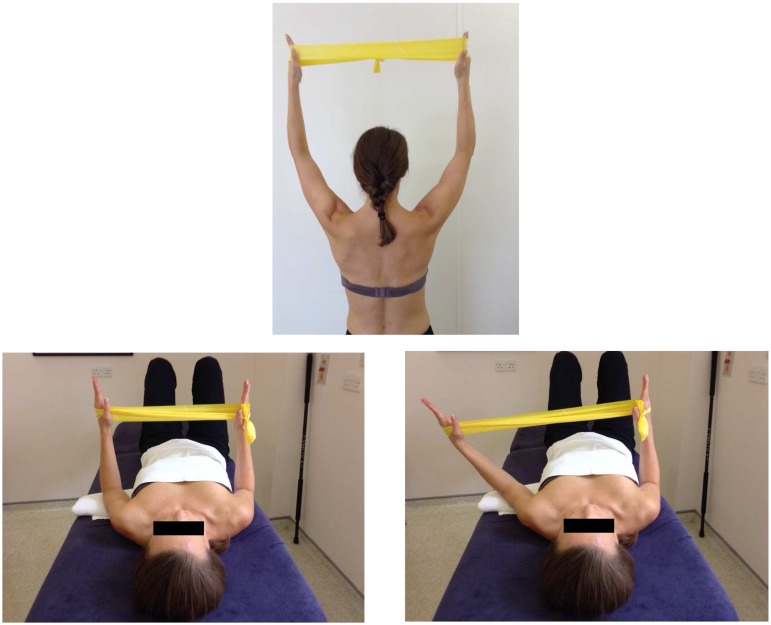
Strengthening external rotation in supine with the scapula controlled (below). Elevation sequencing in, upward shrug with some resistance being used to preset the posterior rotator cuff (above).

Two-point orientation discrimination and cervical kinaesthesia assessment. The dysfunction can become the treatment but should remain non-provocative. Graded Motor Imagery (GMI) may be indicated in the presence of pain-mediated cortical adaptations (http://www.gradedmotorimagery.com ).
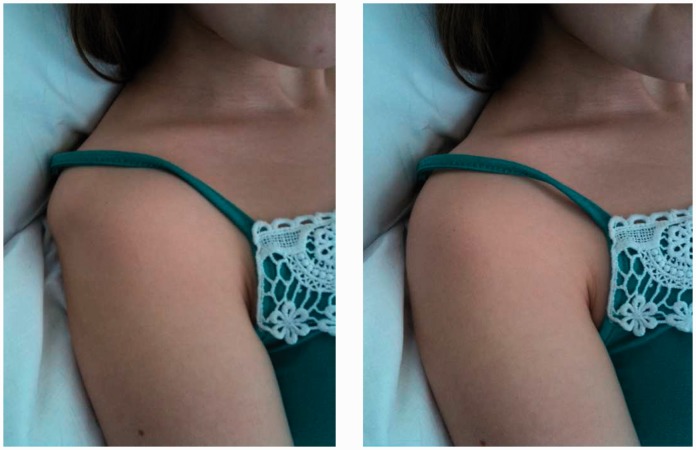
A persistently hypertonic pectoralis major causing anterior subluxation (visible and palpable). Relaxation techniques focusing on pectoralis major control facilitates relocation.
References
-
- Lewis A, Kitamura T, Bayley JIL. Mini symposium: shoulder instability (ii) The classification of shoulder instability: new light through old windows!. Curr Orthop 2004; 18: 97–108.
-
- Neer II CS. Involuntary, inferior and multidirectional instability of the shoulder: etiology, recognition and treatment. J Bone Joint Surg (A) 1980; 62: 897–908. - PubMed
-
- Calvert P. Mini-symposium: shoulder instability classification and clinical assessment. Curr Orthopaed 1996; 10: 151–7.
-
- Kuhn J. A new classification system for shoulder instability. Br J Sports Med 2010; 44: 341–6. - PubMed
-
- McFarland EG, Kim TK, Park HB, Neira CA, Gutierrez MI. The effect of variation in definition on the diagnosis of multidirectional instability of the shoulder. J Bone Joint Surg Am 2003; 85: 2138–44. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources