

Acromial and scapular spine fractures after reverse total shoulder arthroplasty
- PMID: 27583005
- PMCID: PMC4950466
- DOI: 10.1177/1758573216628783
Acromial and scapular spine fractures after reverse total shoulder arthroplasty
Abstract
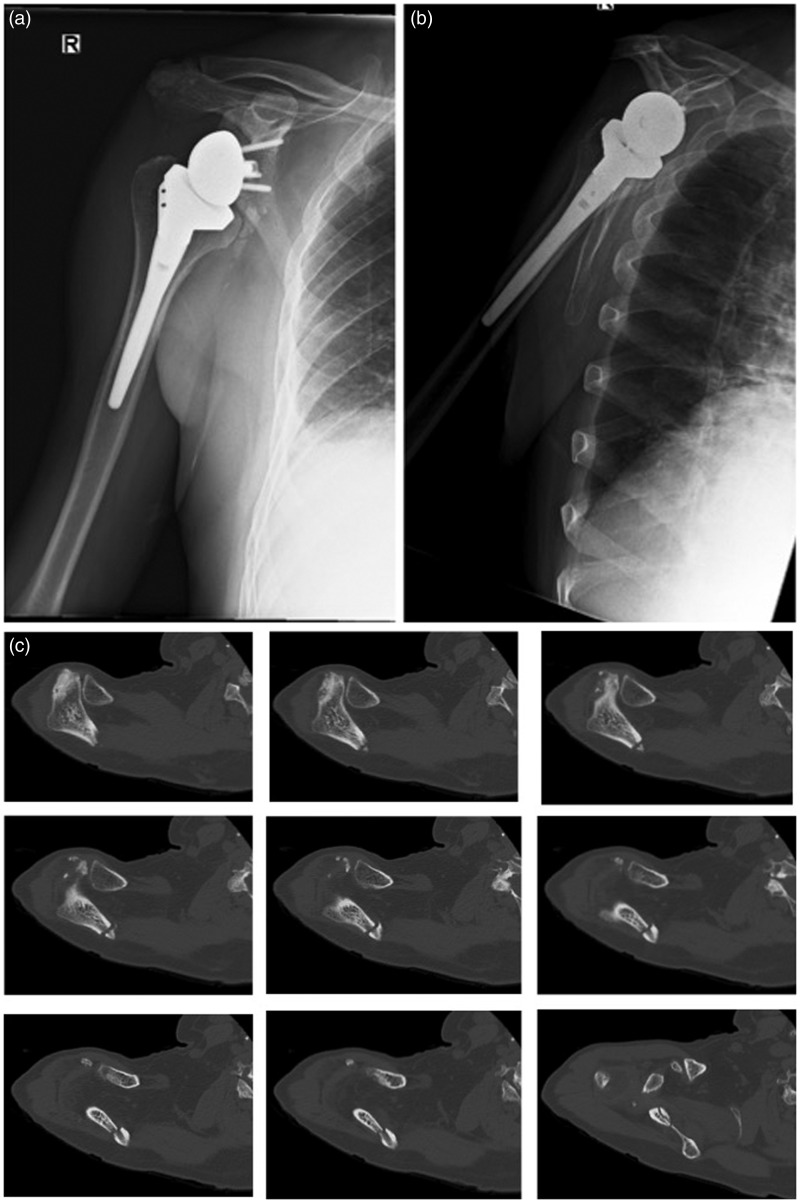
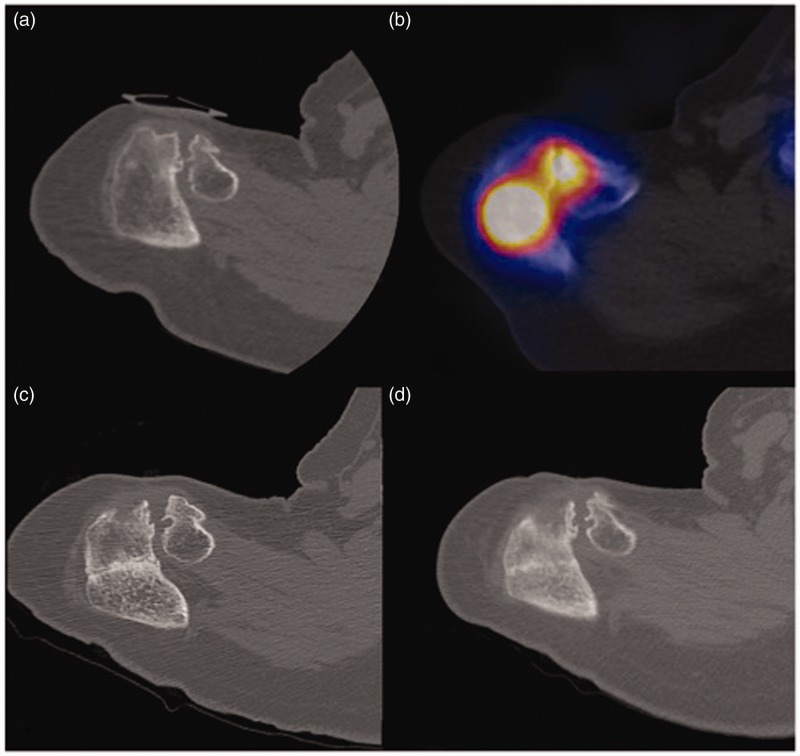
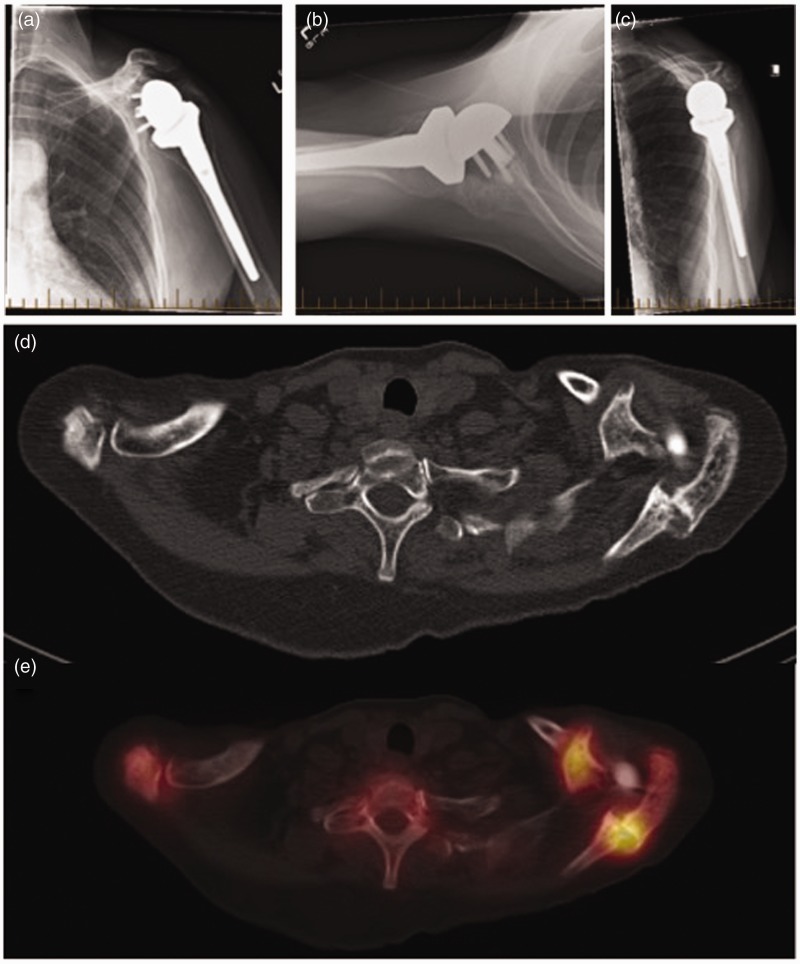
Acromial and scapular spine fractures after reverse total shoulder arthroplasty occur predominantly as a result of bony insufficiency secondary to patient and intra-operative technical factors. The spectrum of the pathology can range from a stress reaction to an undisplaced or displaced fracture. Prompt diagnosis of these fractures requires a high suspicion in the postoperative patient with a clinical presentation of acute onset of pain along the acromion or scapular spine and/or deterioration of shoulder function. Conventional shoulder radiographs are frequently unreliable in identifying these fractures, especially if they are undisplaced. Computed tomography (CT) and/or single photon emission computed tomography/CT scans are useful imaging modalities for obtaining a definitive diagnosis. Early diagnosis and non-operative treatment of a stress reaction or undisplaced fracture is essential for preventing further displacement and potential disability. The management of displaced fractures is challenging for the orthopaedic surgeon as a result of high rates of mal-union or non-union, decreased functional outcomes, and variable results after open reduction and internal fixation. Strategies for preventing these fractures include optimizing the patient's bone health, correct glenoid baseplate screw length and position, and avoiding excessive deltoid tension. Further research is required to identify the specific patient and fracture characteristics that will benefit from conservative versus operative management.
Keywords: acromion; periprosthetic fractures; reverse total shoulder arthroplasty; scapula.
Figures
Similar articles
-
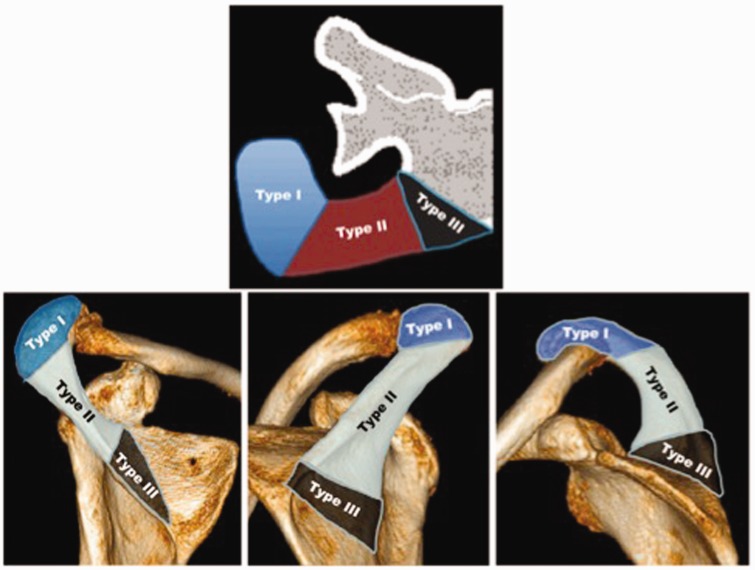
Classification of postoperative acromial fractures following reverse shoulder arthroplasty.J Bone Joint Surg Am. 2013 Aug 7;95(15):e104. doi: 10.2106/JBJS.K.01516. J Bone Joint Surg Am. 2013. PMID: 23925750
-
Clinical results of conservative versus operative treatment of acromial and scapular spine fractures following reverse total shoulder arthroplasty.J Shoulder Elbow Surg. 2022 Oct;31(10):2076-2081. doi: 10.1016/j.jse.2022.03.005. Epub 2022 Apr 18. J Shoulder Elbow Surg. 2022. PMID: 35447315
-
Acromial and Scapular Spine Fractures following Reverse Total Shoulder Arthroplasty-A Systematic Review of Fixation Constructs and Techniques.J Clin Med. 2022 Nov 28;11(23):7025. doi: 10.3390/jcm11237025. J Clin Med. 2022. PMID: 36498600 Free PMC article. Review.
-
How common are acromial and scapular spine fractures after reverse shoulder arthroplasty?: A systematic review.Bone Joint J. 2019 Jun;101-B(6):627-634. doi: 10.1302/0301-620X.101B6.BJJ-2018-1187.R1. Bone Joint J. 2019. PMID: 31154841
-
Causes of acromion and scapular spine fractures following reverse shoulder arthroplasty: a retrospective analysis and literature review.Int Orthop. 2020 Dec;44(12):2673-2681. doi: 10.1007/s00264-020-04813-5. Epub 2020 Sep 29. Int Orthop. 2020. PMID: 32995915 Free PMC article. Review.
Cited by
-
Bilateral atraumatic acromial base fractures following reverse shoulder arthroplasty managed with open reduction and internal fixation: a case report.JSES Int. 2023 Sep 16;8(1):95-98. doi: 10.1016/j.jseint.2023.08.012. eCollection 2024 Jan. JSES Int. 2023. PMID: 38312292 Free PMC article. No abstract available.
-
Is Acromial Fracture after Reverse Total Shoulder Arthroplasty a Negligible Complication?: A Systematic Review.Clin Orthop Surg. 2019 Dec;11(4):427-435. doi: 10.4055/cios.2019.11.4.427. Epub 2019 Nov 12. Clin Orthop Surg. 2019. PMID: 31788166 Free PMC article.
-
Maximizing Muscle Function in Cuff-Deficient Shoulders: A Rehabilitation Proposal for Reverse Arthroplasty.J Shoulder Elb Arthroplast. 2021 Jul 1;5:24715492211023302. doi: 10.1177/24715492211023302. eCollection 2021. J Shoulder Elb Arthroplast. 2021. PMID: 34993379 Free PMC article. Review.
-
Does Preservation of Coracoacromial Ligament Reduce the Acromial Stress Pathology Following Reverse Total Shoulder Arthroplasty?J Shoulder Elb Arthroplast. 2021 Jun 14;5:24715492211022171. doi: 10.1177/24715492211022171. eCollection 2021. J Shoulder Elb Arthroplast. 2021. PMID: 34497968 Free PMC article.
-
The modern reverse shoulder arthroplasty and an updated systematic review for each complication: part II.JSES Int. 2020 Sep 10;5(1):121-137. doi: 10.1016/j.jseint.2020.07.018. eCollection 2021 Jan. JSES Int. 2020. PMID: 33554177 Free PMC article. Review.
References
-
- Boileau P, Gonzalez JF, Chuinard C, et al. Reverse total shoulder arthroplasty after failed rotator cuff surgery. J Shoulder Elbow Surg 2009; 18: 600–6. - PubMed
-
- Matsen FA, III, Boileau P, Walch G, et al. The reverse total shoulder arthroplasty. J Bone Joint Surg Am 2007; 89: 660–7. - PubMed
-
- Wall B, Nové-Josserand L, O’Connor DP, et al. Reverse total shoulder arthroplasty: a review of results according to etiology. J Bone Joint Surg Am 2007; 89: 1476–85. - PubMed
-
- Rittmeister M, Kersch-Baumer F. Grammont reverse total shoulder arthroplasty in patients with rheumatoid arthritis and non reconstructable rotator cuff lesions. J Shoulder Elbow Surg 2001; 10: 17–22. - PubMed
-
- Boileau P, Watkinson DJ, Hatzidakis AM, et al. Grammont reverse prosthesis: design, rationale, and biomechanics. J Shoulder Elbow Surg 2005; 14: 147S–61S. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials