

Towards a neurophysiological signature for fibromyalgia
- PMID: 27583567
- PMCID: PMC5161739
- DOI: 10.1097/j.pain.0000000000000707
Towards a neurophysiological signature for fibromyalgia
Abstract
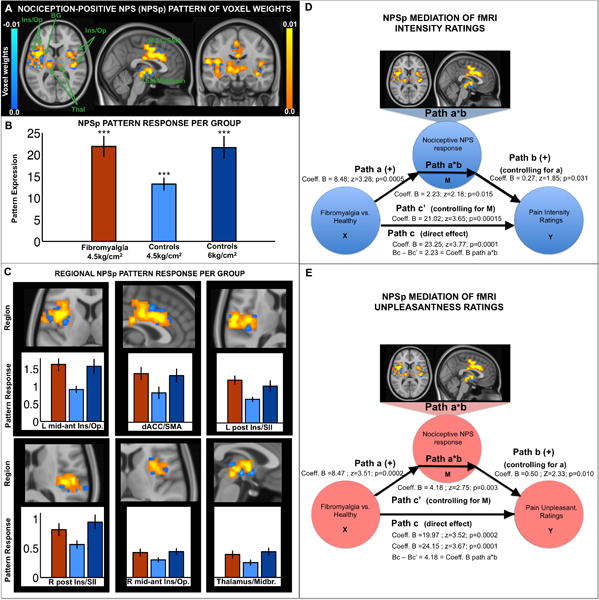
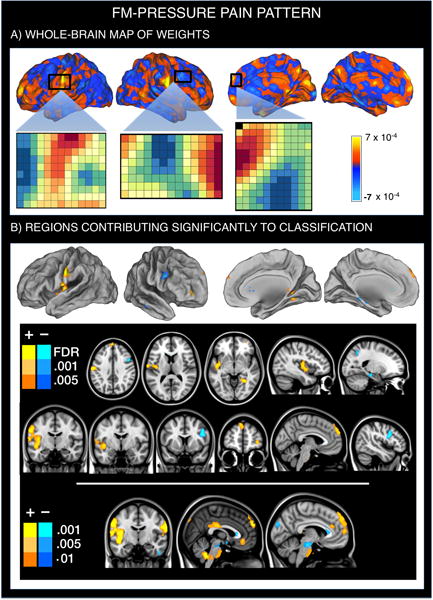
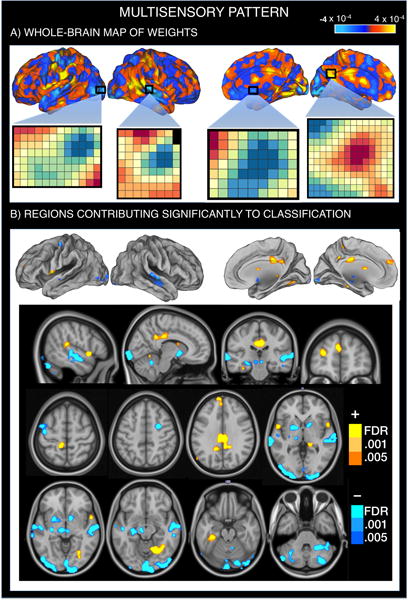
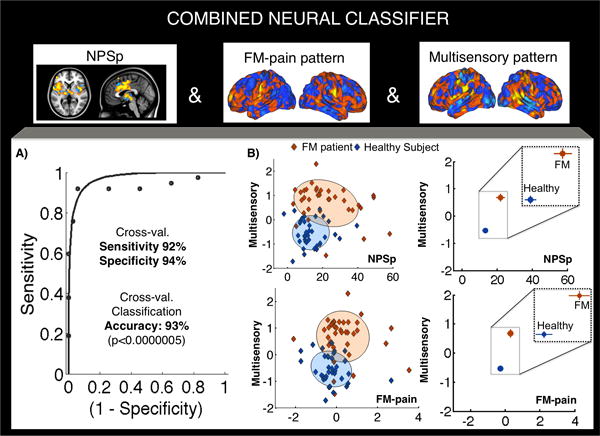
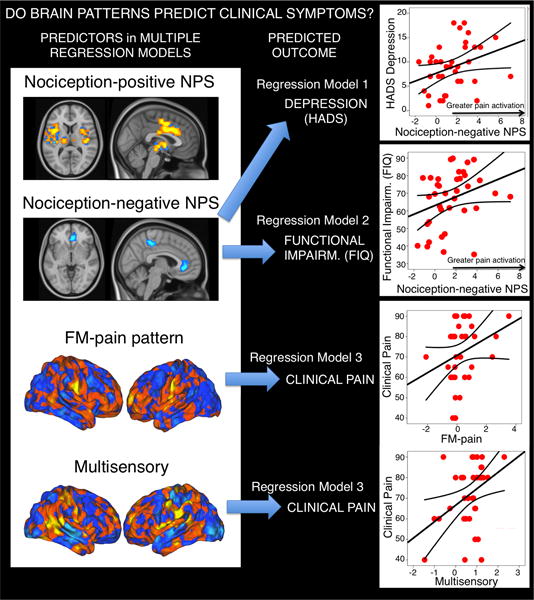
Patients with fibromyalgia (FM) show characteristically enhanced unpleasantness to painful and nonpainful sensations accompanied by altered neural responses. The diagnostic potential of such neural alterations, including their sensitivity and specificity to FM (vs healthy controls) is unknown. We identify a brain signature that characterizes FM central pathophysiology at the neural systems level. We included 37 patients with FM and 35 matched healthy controls, and analyzed functional magnetic resonance imaging responses to (1) painful pressure and (2) nonpainful multisensory (visual-auditory-tactile) stimulation. We used machine-learning techniques to identify a brain-based FM signature. When exposed to the same painful stimuli, patients with FM showed greater neurologic pain signature (NPS; Wager et al., 2013. An fMRI-based neurologic signature of physical pain. N Engl J Med 2013;368:1388-97) responses. In addition, a new pain-related classifier ("FM-pain") revealed augmented responses in sensory integration (insula/operculum) and self-referential (eg, medial prefrontal) regions in FM and reduced responses in the lateral frontal cortex. A "multisensory" classifier trained on nonpainful sensory stimulation revealed augmented responses in the insula/operculum, posterior cingulate, and medial prefrontal regions and reduced responses in the primary/secondary sensory cortices, basal ganglia, and cerebellum. Combined activity in the NPS, FM pain, and multisensory patterns classified patients vs controls with 92% sensitivity and 94% specificity in out-of-sample individuals. Enhanced NPS responses partly mediated mechanical hypersensitivity and correlated with depression and disability (Puncorrected < 0.05); FM-pain and multisensory responses correlated with clinical pain (Puncorrected < 0.05). The study provides initial characterization of individual patients with FM based on pathophysiological, symptom-related brain features. If replicated, these brain features may constitute objective neural targets for therapeutic interventions. The results establish a framework for assessing therapeutic mechanisms and predicting treatment response at the individual level.
Conflict of interest statement
The authors declare no conflict of interests.
Figures
References
-
- Alanoglu E, Ulas UH, Ozdag F, Odabasi Z, Cakci A, Vural O. Auditory event-related brain potentials in fibromyalgia syndrome. Rheumatol Int. 2005;25(5):345–349. - PubMed
-
- Albuquerque RJ, de Leeuw R, Carlson CR, Okeson JP, Miller CS, Andersen AH. Cerebral activation during thermal stimulation of patients who have burning mouth disorder: an fMRI study. Pain. 2006;122(3):223–234. - PubMed
-
- Aparicio VA, Segura-Jimenez V, Alvarez-Gallardo IC, Soriano-Maldonado A, Castro-Pinero J, Delgado-Fernandez M, Carbonell-Baeza A. Fitness Testing in the Fibromyalgia Diagnosis: the al-Andalus Project. Med Sci Sports Exerc. 2014 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
