

Lessons from surgical outcome for intracranial meningioma involving major venous sinus
- PMID: 27583904
- PMCID: PMC5008588
- DOI: 10.1097/MD.0000000000004705
Lessons from surgical outcome for intracranial meningioma involving major venous sinus
Abstract
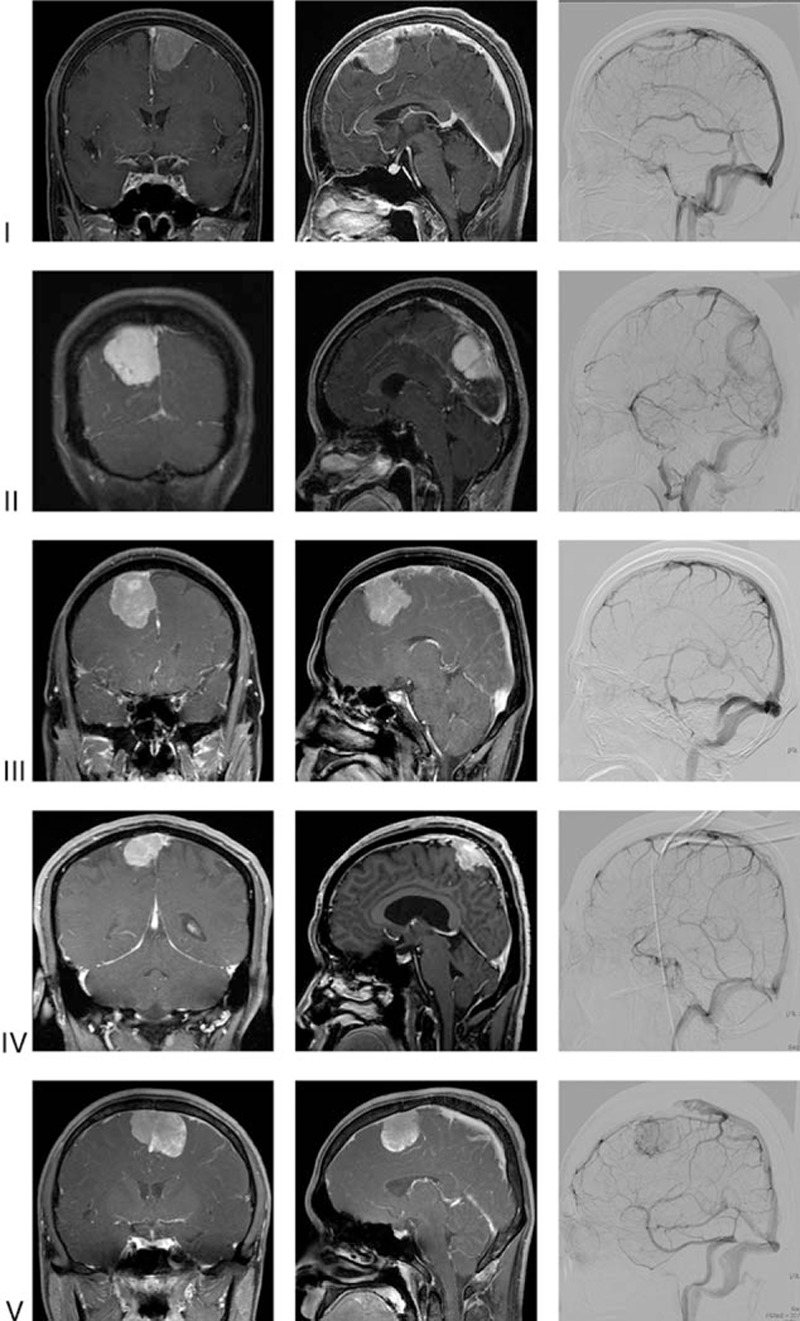
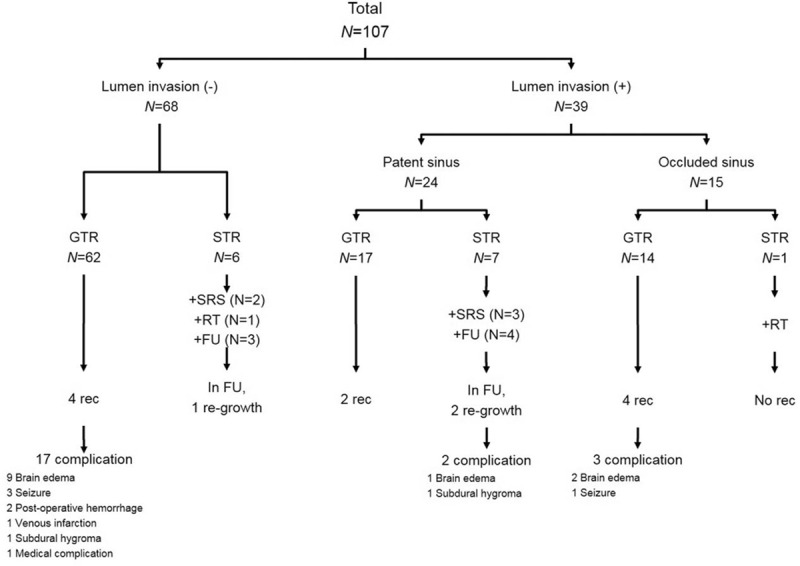
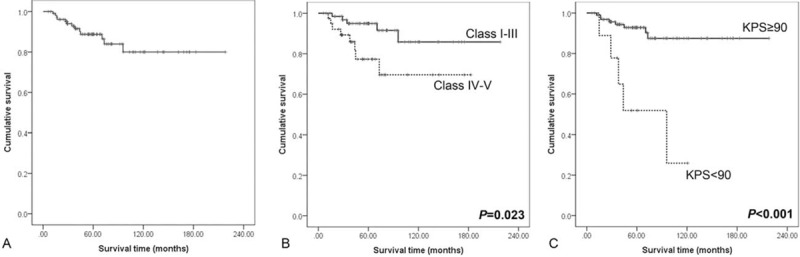
Intracranial meningiomas involving the major venous sinus (MVS) pose several complication risks upon performing radical resection. Some surgeons consider MVS invasion a contraindication for a complete resection of meningioma, and others suggest total resection followed by venous reconstruction. The aim of the study was to analyze our surgical results and discuss management strategy for intracranial meningiomas involving the MVS. Between 1993 and 2011, 107 patients with intracranial meningiomas involving MVS underwent surgery in our institution. Clinicoradiological features including pathological features and operative findings were retrospectively analyzed. Median follow-up duration was 60.2 months (range, 6.2-218.2 months). Distributions of tumor cases according to the involved sinus were as follows: 86% parasagittal, 10.3% tentorial, and 3.7% peritorcular. Simpson Grade I/II removal was achieved in 93 of 107 patients (87%). Partially or totally occluded MVS by their meningiomas (Sindou classification IV and V) was found in 39 patients (36%). Progression rate was 12% (13/107) and progression-free survival rates were 89%, 86%, and 80% at 5, 7, and 10 years, respectively. Sindou classification (IV/V) and Karnofsky performance status (KPS) score 6 month after the surgery (KPS < 90) were predictive factors for progression in our study (P = 0.044 and P = 0.001, respectively). The resection degree did not reach statistical significance (P = 0.484). Interestingly, there was no progression in patients that underwent radiation therapy or gamma knife radiosurgery for residual tumor. There were no perioperative deaths. Complication rate was 21% with brain swelling being the most common complication. There was no predictive factor for occurrence of postoperative complication in this study. In conclusion, complete tumor resection with sinus reconstruction did not significantly prevent tumor recurrence in intracranial meningioma involving MVS. Considering the complications from this procedure as it has possibly related with reduced postoperative KPS score, the tumor should be removed as much as possible while leaving remnant portion with significant invasion of sinus or drainage vein. Following radiation therapy or gamma knife radiosurgery for a remnant or recurred meningioma might then be justified.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Results of attempted radical tumor removal and venous repair in 100 consecutive meningiomas involving the major dural sinuses.J Neurosurg. 2006 Oct;105(4):514-25. doi: 10.3171/jns.2006.105.4.514. J Neurosurg. 2006. PMID: 17044551
-
Meningiomas invading the superior sagittal sinus: surgical experience in 108 cases.Neurosurgery. 2004 Dec;55(6):1263-72; discussion 1272-4. doi: 10.1227/01.neu.0000143373.74160.f2. Neurosurgery. 2004. PMID: 15574208
-
Management of Meningiomas Involving the Major Venous Sinuses: A Single-Institution Experience.World Neurosurg. 2019 Jul;127:e179-e185. doi: 10.1016/j.wneu.2019.03.043. Epub 2019 Mar 13. World Neurosurg. 2019. PMID: 30878750
-
Meningiomas engaging major venous sinuses.World Neurosurg. 2014 Jan;81(1):116-24. doi: 10.1016/j.wneu.2013.01.095. Epub 2013 Jan 30. World Neurosurg. 2014. PMID: 23376533 Review.
-
Optimal surgical strategy for meningiomas involving the superior sagittal sinus: a systematic review.Neurosurg Rev. 2020 Apr;43(2):525-535. doi: 10.1007/s10143-018-1026-1. Epub 2018 Aug 31. Neurosurg Rev. 2020. PMID: 30171502
Cited by
-
Intraoperative MRI for the microsurgical resection of meningiomas close to eloquent areas or dural sinuses: patient series.J Neurosurg Case Lessons. 2021 Feb 22;1(8):CASE20149. doi: 10.3171/CASE20149. eCollection 2021 Feb 22. J Neurosurg Case Lessons. 2021. PMID: 35855309 Free PMC article.
-
Knowledge discovery from database: MRI radiomic features to assess recurrence risk in high-grade meningiomas.BMC Med Imaging. 2025 Jan 9;25(1):14. doi: 10.1186/s12880-024-01483-2. BMC Med Imaging. 2025. PMID: 39780070 Free PMC article.
-
MRI- and DWI-Based Radiomics Features for Preoperatively Predicting Meningioma Sinus Invasion.J Imaging Inform Med. 2024 Jun;37(3):1054-1066. doi: 10.1007/s10278-024-01024-x. Epub 2024 Feb 13. J Imaging Inform Med. 2024. PMID: 38351221 Free PMC article.
-
Predictor factors for recurrence in atypical meningiomas.Rom J Morphol Embryol. 2023 Jul-Sep;64(3):333-342. doi: 10.47162/RJME.64.3.05. Rom J Morphol Embryol. 2023. PMID: 37867351 Free PMC article.
-
Meningioma involving the superior sagittal sinus: long-term outcome after robotic radiosurgery in primary and recurrent situation.Front Oncol. 2023 Jul 11;13:1206059. doi: 10.3389/fonc.2023.1206059. eCollection 2023. Front Oncol. 2023. PMID: 37496660 Free PMC article.
References
-
- Quest DO. Meningiomas: an update. Neurosurgery 1978; 3:219–225. - PubMed
-
- Wara WM, Sheline GE, Newman H, et al. Radiation therapy of meningiomas. Am J Roentgenol Radium Ther Nucl Med 1975; 123:453–458. - PubMed
-
- Sindou M. Meningiomas invading the sagittal or transverse sinuses, resection with venous reconstruction. J Clin Neurosci 2001; 8 suppl 1:8–11. - PubMed
-
- Sindou M, Auque J, Jouanneau E. Neurosurgery and the intracranial venous system. Acta Neurochir Suppl 2005; 94:167–175. - PubMed
-
- Whittle IR, Smith C, Navoo P, et al. Meningiomas. Lancet 2004; 363:1535–1543. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
