

Poor adherence and low persistency rates for hepatocellular carcinoma surveillance in patients with chronic hepatitis B
- PMID: 27583921
- PMCID: PMC5008605
- DOI: 10.1097/MD.0000000000004744
Poor adherence and low persistency rates for hepatocellular carcinoma surveillance in patients with chronic hepatitis B
Abstract
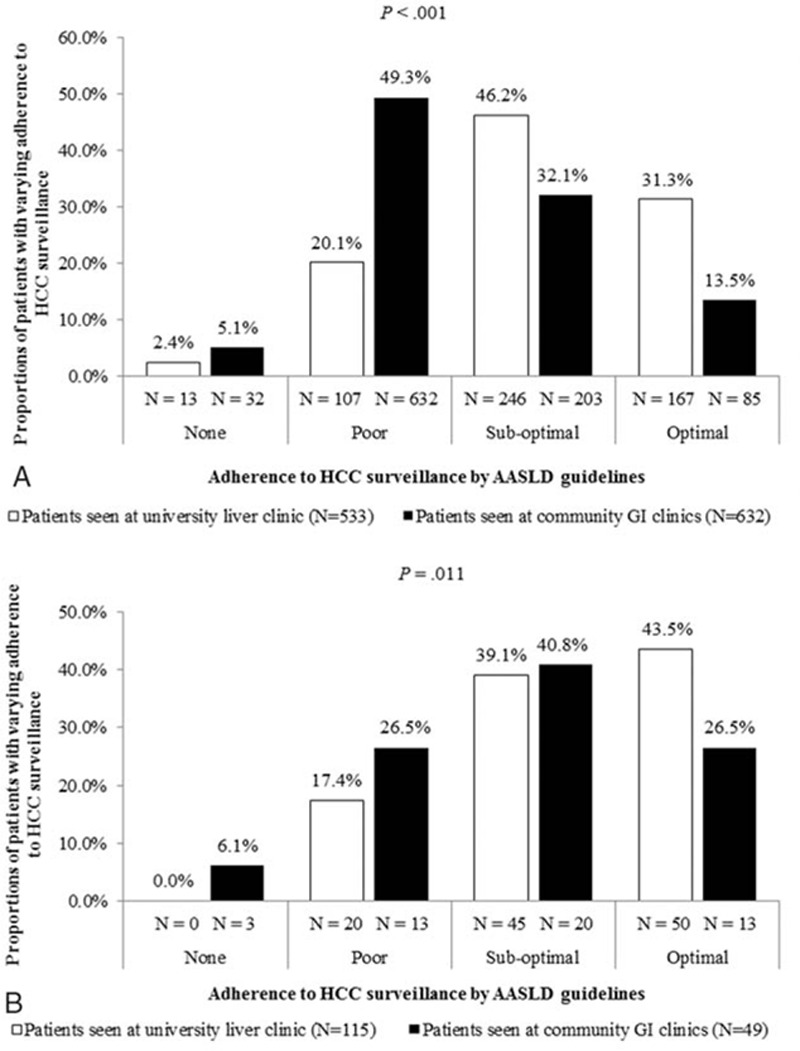
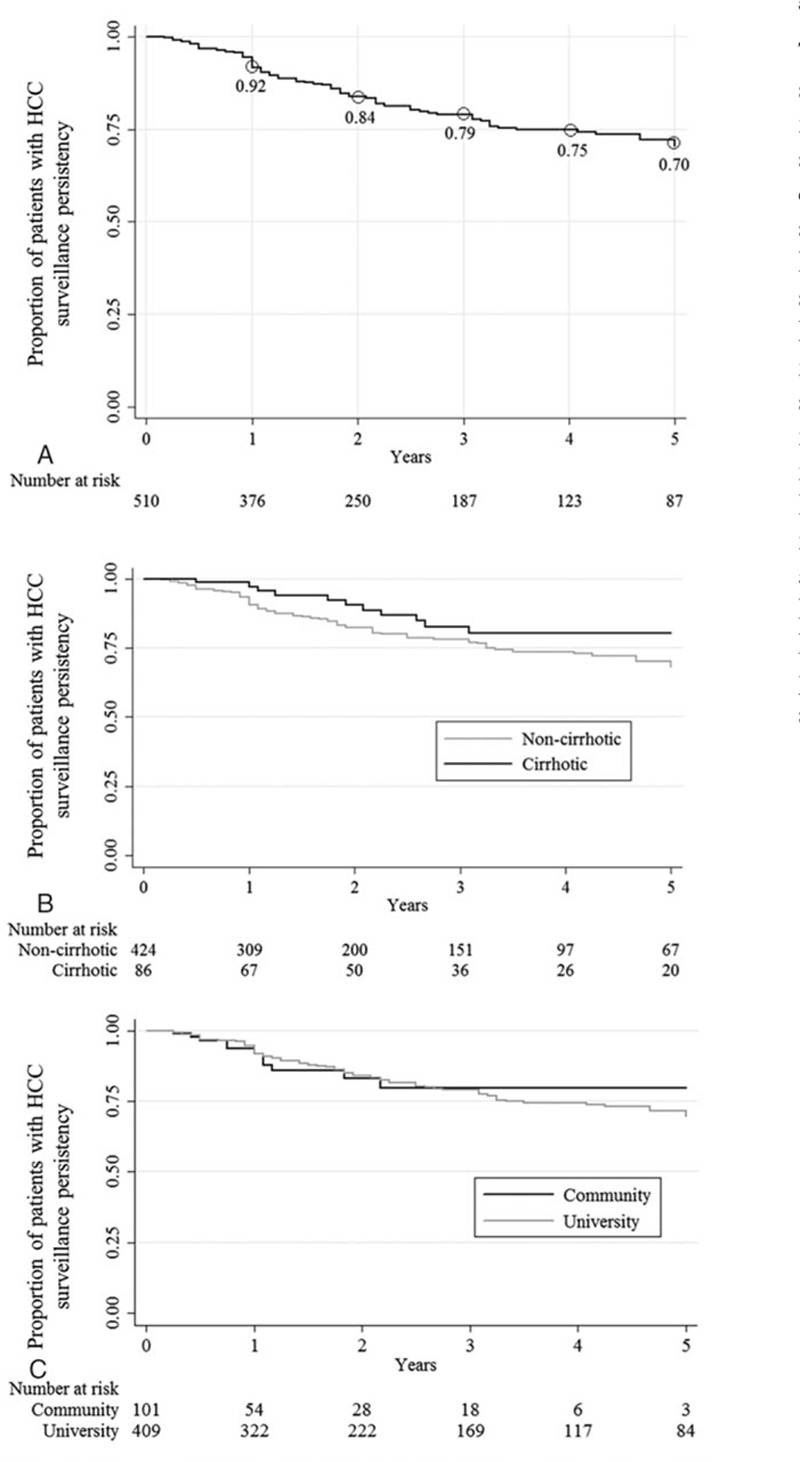
Our goal was to examine rates and predictors for hepatocellular carcinoma (HCC) surveillance adherence and persistency, since studies of such adherence and persistency in patients with chronic hepatitis (CHB) are currently limited.Consecutive CHB patients (N = 1329) monitored for ≥1 year at 4 US clinics from January 1996 to July 2013 were retrospectively studied. Surveillance adherence was evaluated based on the American Association for the Study of Liver Diseases guidelines. Kaplan-Meier method was used to analyze surveillance persistency of 510 patients who had initially fair adherence (having at least annual surveillance imaging with further follow-up).Mean age was 48, with the majority being male (58%), Asian (92%), foreign-born (95%), and medically insured (97%). Patients with cirrhosis and those seen at university liver clinics were more likely to have optimal HCC surveillance than those without cirrhosis and those seen at community clinics (38.4% vs 21.6%, P <0.001 and 33.5% vs 14.4%, P < 0.001, respectively). HCC diagnosed in optimally adherent patients trended toward smaller tumor size (P < 0.08). On multivariate analysis also inclusive of age, sex, clinical visits, cirrhosis, clinic setting and antiviral therapy use, strong independent predictors for having at least annual imaging were a history of more frequent clinical visits (odds ratio [OR] = 2.5, P < 0.001) and university-based care (OR = 5.2, P < 0.001). Even for those with initially fair adherence, persistency dropped to 70% at 5 years.Adherence and persistency to HCC surveillance in CHB patients is generally poor. More frequent clinic visits and university-based settings were significant and strong predictors of at least annual HCC surveillance adherence.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

Similar articles
-
Adherence to screening for hepatocellular carcinoma among patients with cirrhosis or chronic hepatitis B in a community setting.Dig Dis Sci. 2009 Dec;54(12):2712-21. doi: 10.1007/s10620-009-1015-x. Epub 2009 Oct 30. Dig Dis Sci. 2009. PMID: 19876735
-
Hepatocellular carcinoma screening and surveillance in 2293 chronic hepatitis B patients in an endemic area.World J Gastroenterol. 2016 Sep 14;22(34):7806-12. doi: 10.3748/wjg.v22.i34.7806. World J Gastroenterol. 2016. PMID: 27678364 Free PMC article.
-
Poor adherence to hepatocellular carcinoma surveillance: A systematic review and meta-analysis of a complex issue.Liver Int. 2018 Mar;38(3):503-514. doi: 10.1111/liv.13555. Epub 2017 Sep 9. Liver Int. 2018. PMID: 28834146
-
Predictors of failure to detect early hepatocellular carcinoma in patients with chronic hepatitis B who received regular surveillance.Aliment Pharmacol Ther. 2018 Apr;47(8):1201-1212. doi: 10.1111/apt.14578. Epub 2018 Feb 28. Aliment Pharmacol Ther. 2018. PMID: 29492988
-
Prediction models of hepatocellular carcinoma development in chronic hepatitis B patients.World J Gastroenterol. 2016 Oct 7;22(37):8314-8321. doi: 10.3748/wjg.v22.i37.8314. World J Gastroenterol. 2016. PMID: 27729738 Free PMC article. Review.
Cited by
-
Rate of hepatocellular carcinoma surveillance remains low for a large, real-life cohort of patients with hepatitis C cirrhosis.BMJ Open Gastroenterol. 2018 Mar 20;5(1):e000192. doi: 10.1136/bmjgast-2017-000192. eCollection 2018. BMJ Open Gastroenterol. 2018. PMID: 29607053 Free PMC article.
-
Non-cirrhotic hepatocellular carcinoma in chronic viral hepatitis: Current insights and advancements.World J Gastroenterol. 2021 Jun 28;27(24):3466-3482. doi: 10.3748/wjg.v27.i24.3466. World J Gastroenterol. 2021. PMID: 34239263 Free PMC article. Review.
-
Reduced liver cancer mortality with regular clinic follow-up among patients with chronic hepatitis B: A nationwide cohort study.Cancer Med. 2020 Oct;9(20):7781-7791. doi: 10.1002/cam4.3421. Epub 2020 Aug 28. Cancer Med. 2020. PMID: 32857923 Free PMC article.
-
A Retrospective Analysis of Surveillance Adherence of Patients after Treatment of Primary Cutaneous Melanoma.J Clin Aesthet Dermatol. 2017 Dec;10(12):44-48. Epub 2017 Dec 1. J Clin Aesthet Dermatol. 2017. PMID: 29399266 Free PMC article.
-
Baseline assessment of and linkage to care for newly diagnosed patients with chronic hepatitis B.Can Liver J. 2020 Aug 20;3(3):263-275. doi: 10.3138/canlivj.2019-0024. eCollection 2020 Summer. Can Liver J. 2020. PMID: 35992529 Free PMC article.
References
-
- Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011; 61:69–90. - PubMed
-
- Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin 2015; 65:87–108. - PubMed
-
- Cabrera R, Nelson DR. Review article: the management of hepatocellular carcinoma. Aliment Pharmacol Ther 2010; 31:461–476. - PubMed
-
- European Association For The Study Of The Liver. EASL–EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 2012; 56:908–943. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin 2016; 66:7–30. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
