

End-of-life care in patients with advanced lung cancer
- PMID: 27585597
- PMCID: PMC5933619
- DOI: 10.1177/1753465816660925
End-of-life care in patients with advanced lung cancer
Abstract
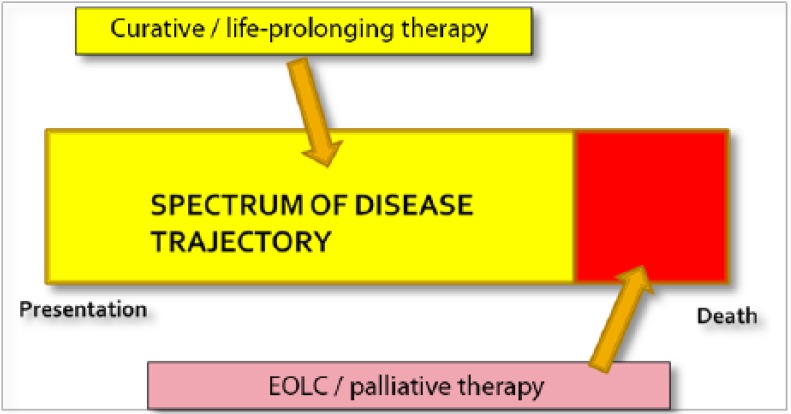
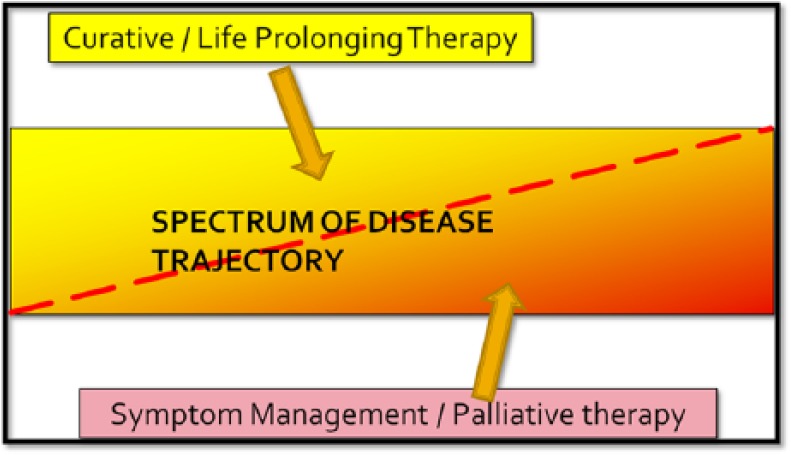
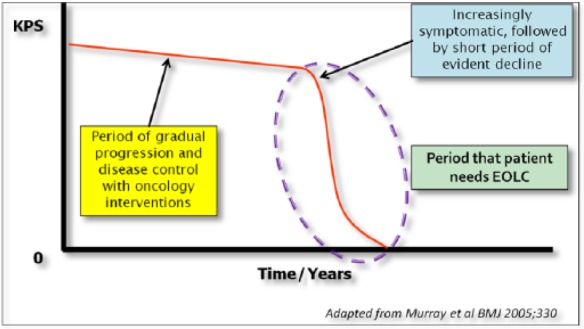
Despite advances in the detection, pathological diagnosis and therapeutics of lung cancer, many patients still develop advanced, incurable and progressively fatal disease. As physicians, the duties to cure sometimes, relieve often and comfort always should be a constant reminder to us of the needs that must be met when caring for a patient with lung cancer. Four key areas of end-of-life care in advanced lung cancer begin with first recognizing 'when a patient is approaching the end of life'. The clinician should be able to recognize when the focus of care needs to shift from an aggressive life-sustaining approach to an approach that helps prepare and support a patient and family members through a period of progressive, inevitable decline. Once the needs are recognized, the second key area is appropriate communication, where the clinician should assist patients and family members in understanding where they are in the disease trajectory and what to expect. This involves developing rapport, breaking bad news, managing expectations and navigating care plans. Subsequently, the third key area is symptom management that focuses on the goals to first and foremost provide comfort and dignity. Symptoms that are common towards the end of life in lung cancer include pain, dyspnoea, delirium and respiratory secretions. Such symptoms need to be anticipated and addressed promptly with appropriate medications and explanations to the patient and family. Lastly, in order for physicians to provide quality end-of-life care, it is necessary to understand the ethical principles applied to end-of-life-care interventions. Misconceptions about euthanasia versus withholding or withdrawing life-sustaining treatments may lead to physician distress and inappropriate decision making.
Keywords: hospice care; lung neoplasm; medical ethics; palliative care; physician–patient relations; terminal care.
© The Author(s), 2016.
Conflict of interest statement
Figures
Similar articles
-
[A position paper on end of life shared between those who believe and those who don't believe: a dialogue is possible].Recenti Prog Med. 2015 Nov;106(11):535-7. doi: 10.1701/2074.22482. Recenti Prog Med. 2015. PMID: 26668036 Italian.
-
[Palliative care in the cardiac setting: a consensus document of the Italian Society of Cardiology/Italian Society of Palliative Care (SIC/SICP)].G Ital Cardiol (Rome). 2019 Jan;20(1):46-61. doi: 10.1714/3079.30720. G Ital Cardiol (Rome). 2019. PMID: 30638215 Italian.
-
Advanced lung disease: quality of life and role of palliative care.Mt Sinai J Med. 2009 Feb;76(1):63-70. doi: 10.1002/msj.20091. Mt Sinai J Med. 2009. PMID: 19170219
-
Ethical decision making with end-of-life care: palliative sedation and withholding or withdrawing life-sustaining treatments.Mayo Clin Proc. 2010 Oct;85(10):949-54. doi: 10.4065/mcp.2010.0201. Epub 2010 Aug 30. Mayo Clin Proc. 2010. PMID: 20805544 Free PMC article. Review.
-
Palliative care and pain management.Med Clin North Am. 2006 Sep;90(5):983-1004. doi: 10.1016/j.mcna.2006.05.016. Med Clin North Am. 2006. PMID: 16962853 Review.
Cited by
-
Rh-endostatin plus camrelizumab and chemotherapy in first-line treatment of advanced non-small cell lung cancer: A multicenter retrospective study.Cancer Med. 2023 Apr;12(7):7724-7733. doi: 10.1002/cam4.5526. Epub 2022 Dec 9. Cancer Med. 2023. PMID: 36494905 Free PMC article.
-
Antitumorigenic Effect of Cannabidiol in Lung Cancer: What Do We Know So Far?–A Mini Review.Iran Biomed J. 2022 Nov 1;26(6):406-13. doi: 10.52547/ibj.3732. Iran Biomed J. 2022. PMID: 36437760 Free PMC article. Review.
-
Family-oriented dignity therapy for patients with lung cancer undergoing chemotherapy: How does it work better?Asia Pac J Oncol Nurs. 2022 Nov 17;10(1):100168. doi: 10.1016/j.apjon.2022.100168. eCollection 2023 Jan. Asia Pac J Oncol Nurs. 2022. PMID: 36578350 Free PMC article.
-
Influence of respiratory function training under the mode of mutual-assisted patients on postoperative pulmonary infection and immune function on lung cancer.Am J Transl Res. 2021 Aug 15;13(8):9260-9268. eCollection 2021. Am J Transl Res. 2021. PMID: 34540042 Free PMC article.
-
Appetite and its association with mortality in patients with advanced cancer - a Post-hoc Analysis from the Palliative D-study.BMC Palliat Care. 2023 Oct 26;22(1):159. doi: 10.1186/s12904-023-01287-1. BMC Palliat Care. 2023. PMID: 37880704 Free PMC article.
References
-
- Ackermann R. (2000) Withholding and withdrawing life-sustaining treatment. Am Fam Physician 62: 1555–1560. - PubMed
-
- Baranzke H. (2012) ‘Sanctity-of-life’—a bioethical principle for a right to life? Ethic Theory Moral Prac 15: 295–308.
-
- Boly M., Faymonville M., Schnakers C., Peigneux P., Lambermont B., Philips C. (2008) Perception of pain in the minimally conscious state with PET activation: an observational study. Lancet Neurol 7: 1013–1020. - PubMed
-
- Breitbart W., Alici Y. (2008) Agitation and delirium at the end of life: ‘We couldn’t manage him.’ JAMA 300: 2898–2910. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
