

Long term outcome of Aldosteronism after target treatments
- PMID: 27586402
- PMCID: PMC5009379
- DOI: 10.1038/srep32103
Long term outcome of Aldosteronism after target treatments
Erratum in
-
Corrigendum: Long term outcome of Aldosteronism after target treatments.Sci Rep. 2017 Mar 24;7:45249. doi: 10.1038/srep45249. Sci Rep. 2017. PMID: 28338668 Free PMC article. No abstract available.
Abstract
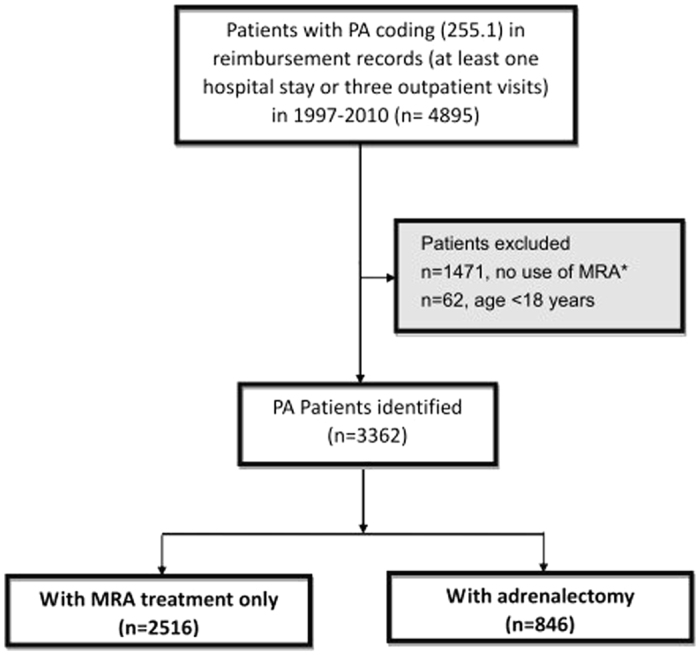
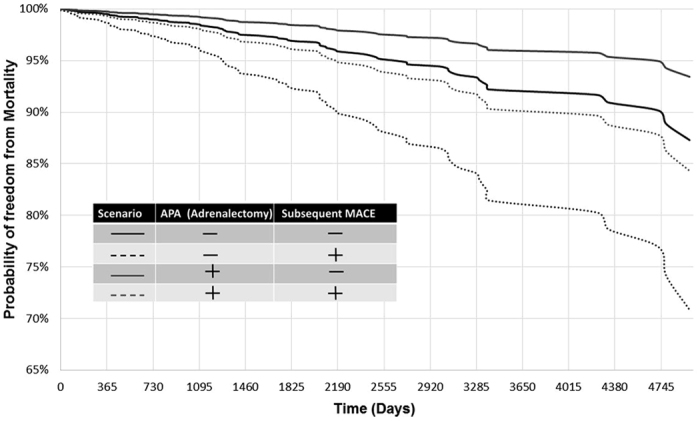
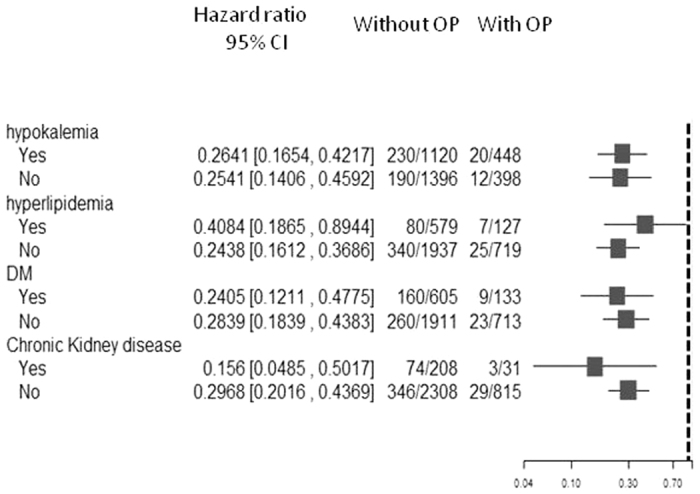
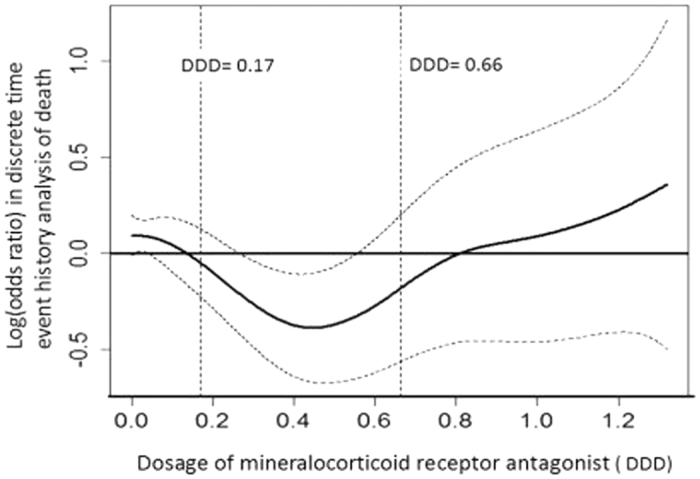
There exists a great knowledge gap in terms of long-term effects of various surgical and pharmacological treatments on outcomes among primary aldosteronism (PA) patients. Using a validated algorithm, we extracted longitudinal data for all PA patients diagnosed in 1997-2010 and treated in the Taiwan National Health Insurance. We identified 3362 PA patients for whom the mean length of follow-up was 5.75 years. PA has higher major cardiovascular events (MACE) than essential hypertension (23.3% vs 19.3%, p = 0.015). Results from the Cox model suggest a strong effect of adrenalectomy on lowering mortality (HR = 0.23 with residual hypertension and 0.21 with resolved hypertension). While the need for mineralocorticoid receptor antagonist (MRA) after diagnosis suggests that a defined daily dose (DDD) of MRA between 12.5 and 50 mg may alleviate risk of death in a U-shape pattern. A specificity test identified patients who has aldosterone producing adenoma (HR = 0.50, p = 0.005) also confirmed adrenalectomy attenuated all-cause mortality. Adrenalectomy decreases long-term all-cause mortality independently from PA cure from hypertension. Prescription corresponding to a DDD between 12.5 and 50 mg may decrease mortality for patients needing MRA. It calls for more attention on early diagnosis, early treatment and prescription of appropriate dosage of MRA for PA patients.
Figures
References
-
- Funder J. W. et al. Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 93, 3266–3281 (2008). - PubMed
-
- Milliez P. et al. Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. Journal of the American College of Cardiology 45, 1243–1248 (2005). - PubMed
-
- Reincke M. et al. Observational study mortality in treated primary aldosteronism: the German Conn’s registry. Hypertension 60, 618–624 (2012). - PubMed
-
- Lin Y. H. et al. Adrenalectomy improves increased carotid intima-media thickness and arterial stiffness in patients with aldosterone producing adenoma. Atherosclerosis 221, 154–159 (2012). - PubMed
-
- Wu V. C. et al. Primary aldosteronism: changes in cystatin C-based kidney filtration, proteinuria, and renal duplex indices with treatment. J Hypertens 29, 1778–1786 (2011). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
