The Association between End-of-Life Care and the Time Interval between Provision of a Do-Not-Resuscitate Consent and Death in Cancer Patients in Korea
- PMID: 27586675
- PMCID: PMC5398395
- DOI: 10.4143/crt.2016.073
The Association between End-of-Life Care and the Time Interval between Provision of a Do-Not-Resuscitate Consent and Death in Cancer Patients in Korea
Abstract
Purpose: We explored the relationship between the use of each medical intervention and the length of time between do-not-resuscitate (DNR) consent and death in Korea.
Materials and methods: A total of 295 terminal cancer patients participated in this retrospective study. Invasive interventions (e.g., cardiopulmonary resuscitation, intubation, and hemodialysis), less invasive interventions (e.g., transfusion, antibiotic use, inotropic use, and laboratory tests), and the time interval between the DNR order and death were evaluated. The subjects were divided into three groups based on the amount of time between DNR consent and death (G1, time interval ≤ 1 day; G2, time interval > 1 day to ≤ 3 days; and G3, time interval > 3 days).
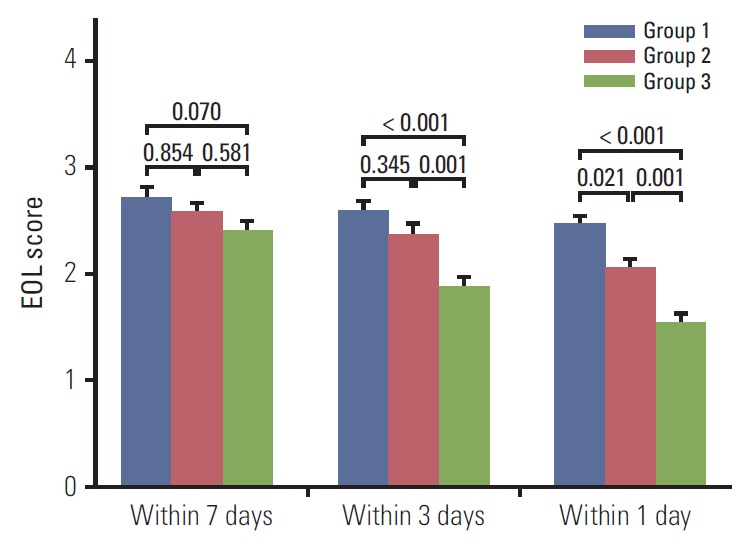
Results: In general, there were fewer transfusions and laboratory tests near death. Invasive interventions tended to be implemented only in the G1 group. There was also less inotrope use and fewer laboratory tests in the G3 group than G1 and G2. Moreover, the G3 group received fewer less invasive interventions than those in G1 (odds ratio [OR], 0.16; 95% confidence interval [CI], 0.03 to 0.84; 3 days before death, and OR, 0.16; 95% CI, 0.04 to 0.59; the day before death). The frequency of less invasive interventions both 1 and 3 days before death was significantly lower for the G3 group than the G1 (p ≤ 0.001) and G2 group compared to G1 (p=0.001).
Conclusion: Earlier attainment of DNR permission was associated with reduced use of medical intervention. Thus, physicians should discuss death with terminal cancer patients at the earliest practical time to prevent unnecessary and uncomfortable procedures and reduce health care costs.
Keywords: Neoplasms; Resuscitation orders; Terminal care.
Conflict of interest statement
Conflict of interest relevant to this article was not reported.
Figures
References
-
- Jonsson PV, McNamee M, Campion EW. The 'Do not resuscitate' order: a profile of its changing use. Arch Intern Med. 1988;148:2373–5. - PubMed
-
- Rabkin MT, Gillerman G, Rice NR. Orders not to resuscitate. N Engl J Med. 1976;295:364–6. - PubMed
-
- Oh DY, Kim JE, Lee CH, Lim JS, Jung KH, Heo DS, et al. Discrepancies among patients, family members, and physicians in Korea in terms of values regarding the withholding of treatment from patients with terminal malignancies. Cancer. 2004;100:1961–6. - PubMed
-
- Kim DY, Lee KE, Nam EM, Lee HR, Lee KW, Kim JH, et al. Do-not-resuscitate orders for terminal patients with cancer in teaching hospitals of Korea. J Palliat Med. 2007;10:1153–8. - PubMed
-
- Oh DY, Kim JH, Kim DW, Im SA, Kim TY, Heo DS, et al. CPR or DNR? End-of-life decision in Korean cancer patients: a single center's experience. Support Care Cancer. 2006;14:103–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical