

Eye Globe Abnormalities on MR and CT in Adults: An Anatomical Approach
- PMID: 27587955
- PMCID: PMC5007393
- DOI: 10.3348/kjr.2016.17.5.664
Eye Globe Abnormalities on MR and CT in Adults: An Anatomical Approach
Abstract
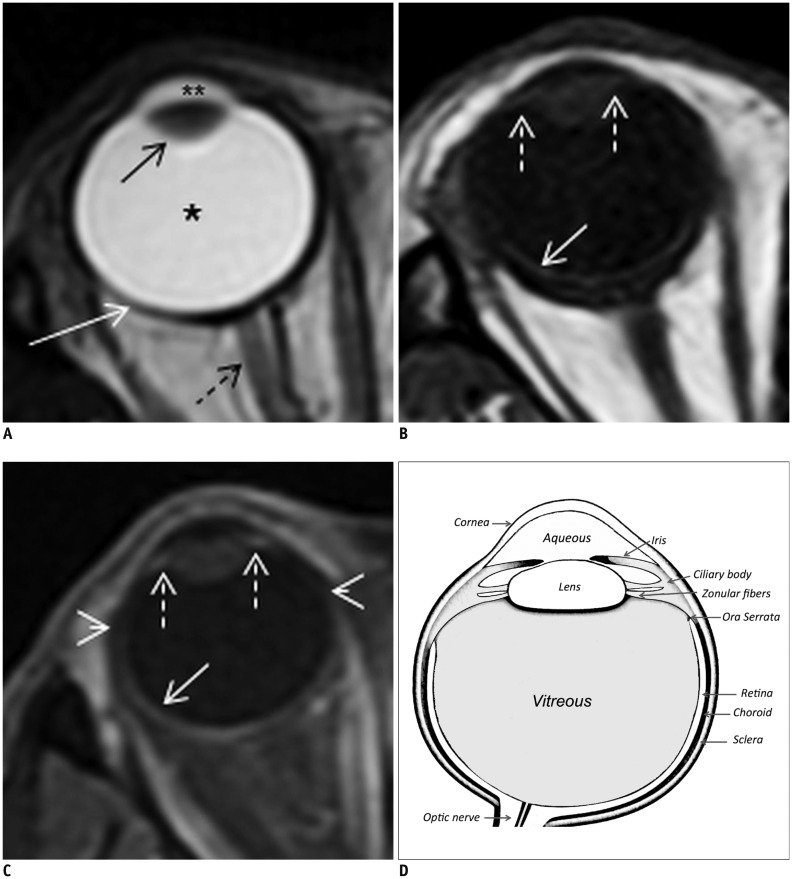
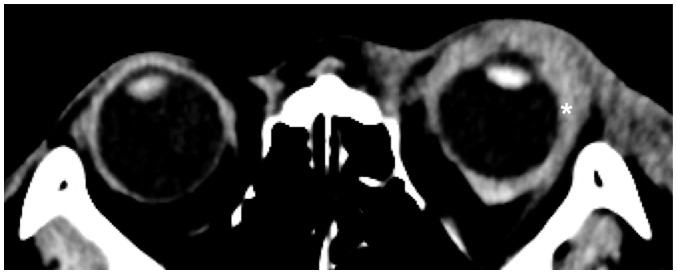
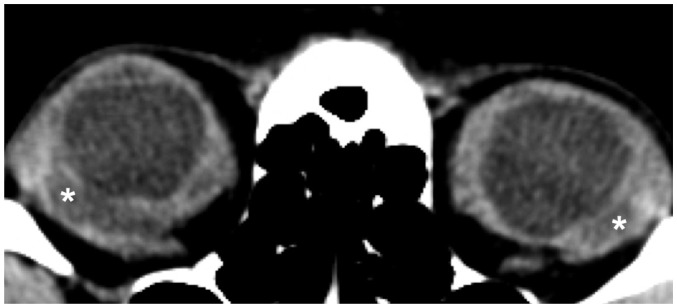
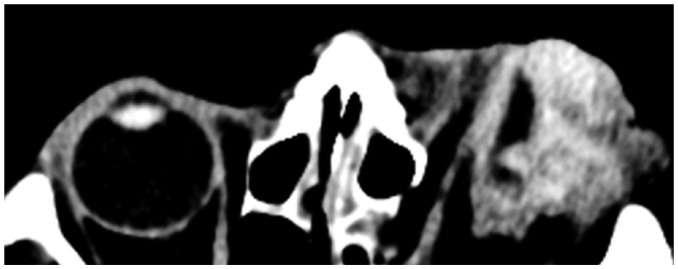
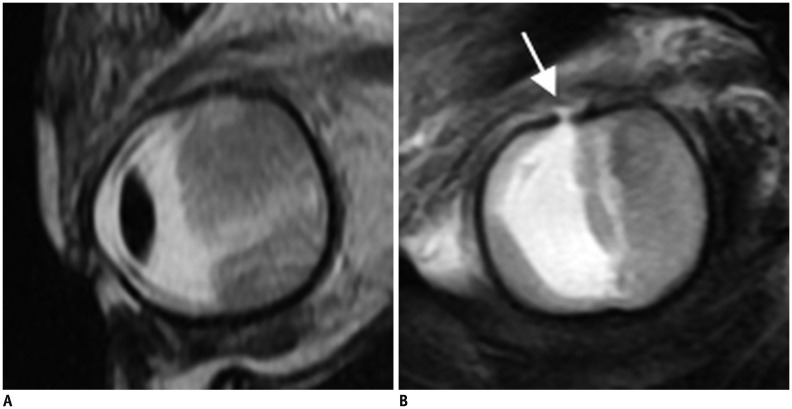
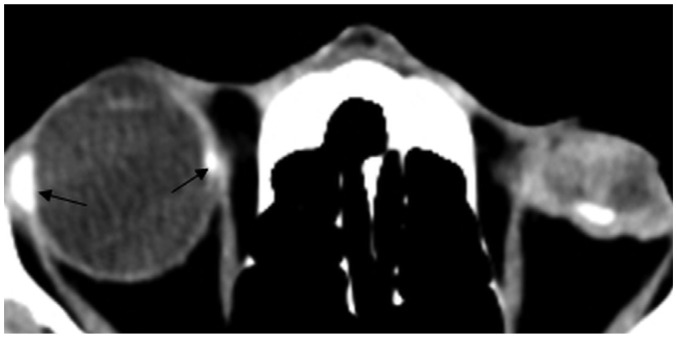
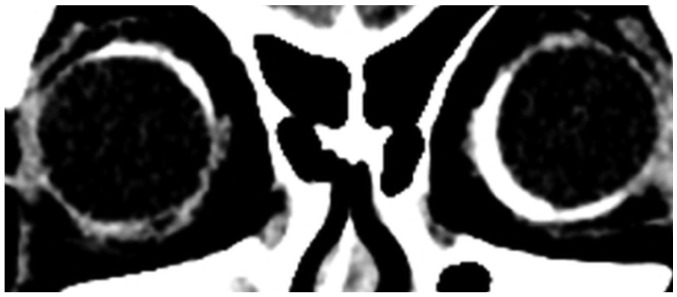
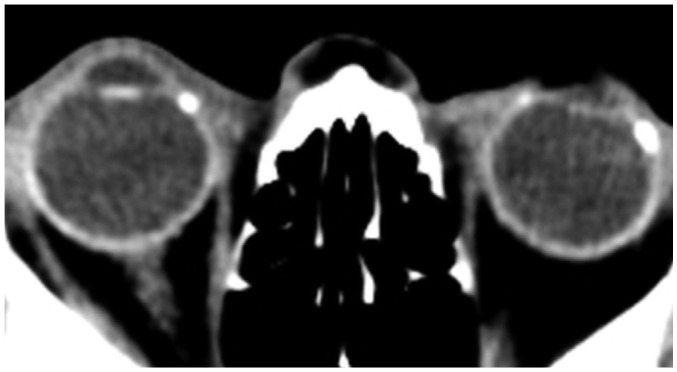
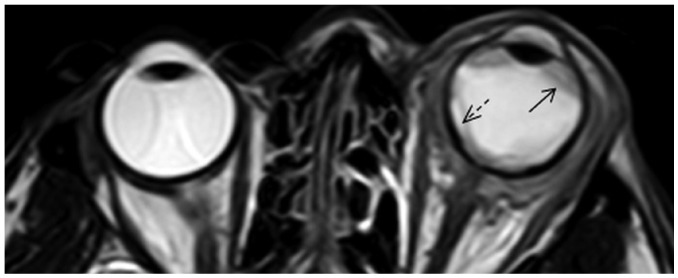
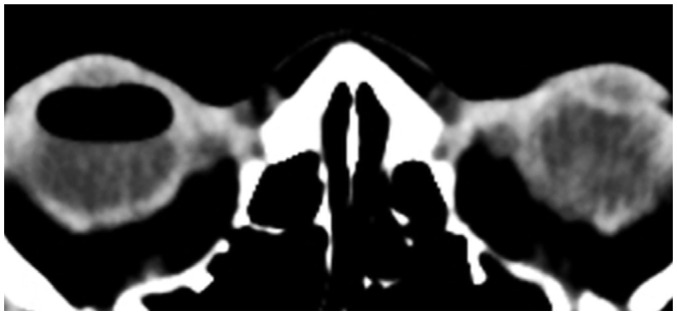
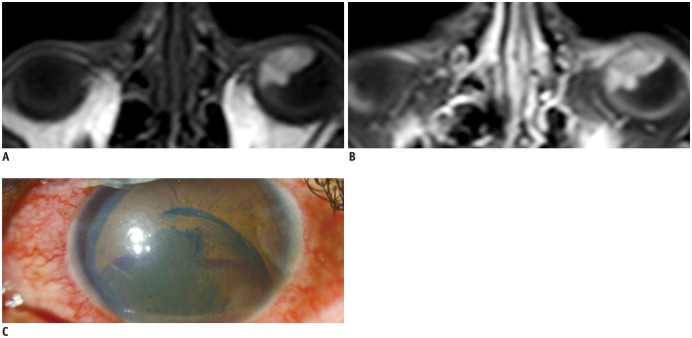
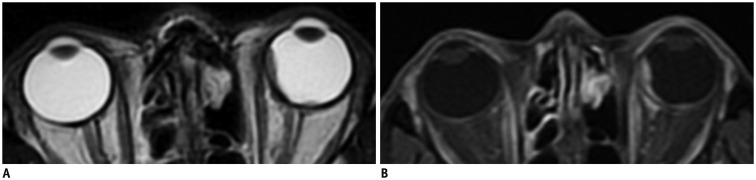
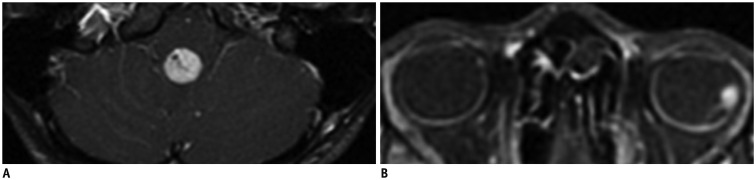
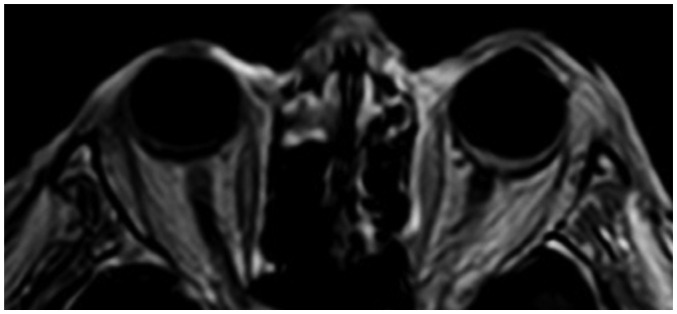
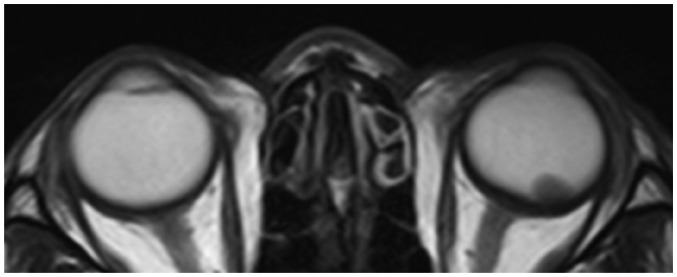
Eye globe abnormalities can be readily detected on dedicated and non-dedicated CT and MR studies. A primary understanding of the globe anatomy is key to characterising both traumatic and non-traumatic globe abnormalities. The globe consists of three primary layers: the sclera (outer), uvea (middle), and retina (inner layer). The various pathological processes involving these layers are highlighted using case examples with fundoscopic correlation where appropriate. In the emergent setting, trauma can result in hemorrhage, retinal/choroidal detachment and globe rupture. Neoplasms and inflammatory/infective processes predominantly occur in the vascular middle layer. The radiologist has an important role in primary diagnosis contributing to appropriate ophthalmology referral, thereby preventing devastating consequences such as vision loss.
Keywords: CT; Eye globe; MRI; Trauma.
Figures


References
-
- Roy AA, Davagnanam I, Evanson J. Abnormalities of the globe. Clin Radiol. 2012;67:1011–1022. - PubMed
-
- Van Tassel P, Mafee MF, Atlas SW, Galetta SL. Chapter 23. Eye, orbit and visual system. In: Atlas SW, editor. Magnetic resonance imaging of the brain and spine. 4th ed. Volume 2. Philadelphia: Lippincott Williams & Wilkins; 2009. pp. 1258–1363.
-
- Mafee MF, Karimi A, Shah J, Rapoport M, Ansari SA. Anatomy and pathology of the eye: role of MR imaging and CT. Neuroimaging Clin N Am. 2005;15:23–47. - PubMed
-
- Goh PS, Gi MT, Charlton A, Tan C, Gangadhara Sundar JK, Amrith S. Review of orbital imaging. Eur J Radiol. 2008;66:387–395. - PubMed
-
- Lane JI, Watson RE, Jr, Witte RJ, McCannel CA. Retinal detachment: imaging of surgical treatments and complications. Radiographics. 2003;23:983–994. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
