

Racial and Ethnic Differences in End-of-Life Medicare Expenditures
- PMID: 27588580
- PMCID: PMC5237584
- DOI: 10.1111/jgs.14263
Racial and Ethnic Differences in End-of-Life Medicare Expenditures
Abstract
Objectives: To determine to what extent demographic, social support, socioeconomic, geographic, medical, and End-of-Life (EOL) planning factors explain racial and ethnic variation in Medicare spending during the last 6 months of life.
Design: Retrospective cohort study.
Setting: Health and Retirement Study (HRS).
Participants: Decedents who participated in HRS between 1998 and 2012 and previously consented to survey linkage with Medicare claims (N = 7,105).
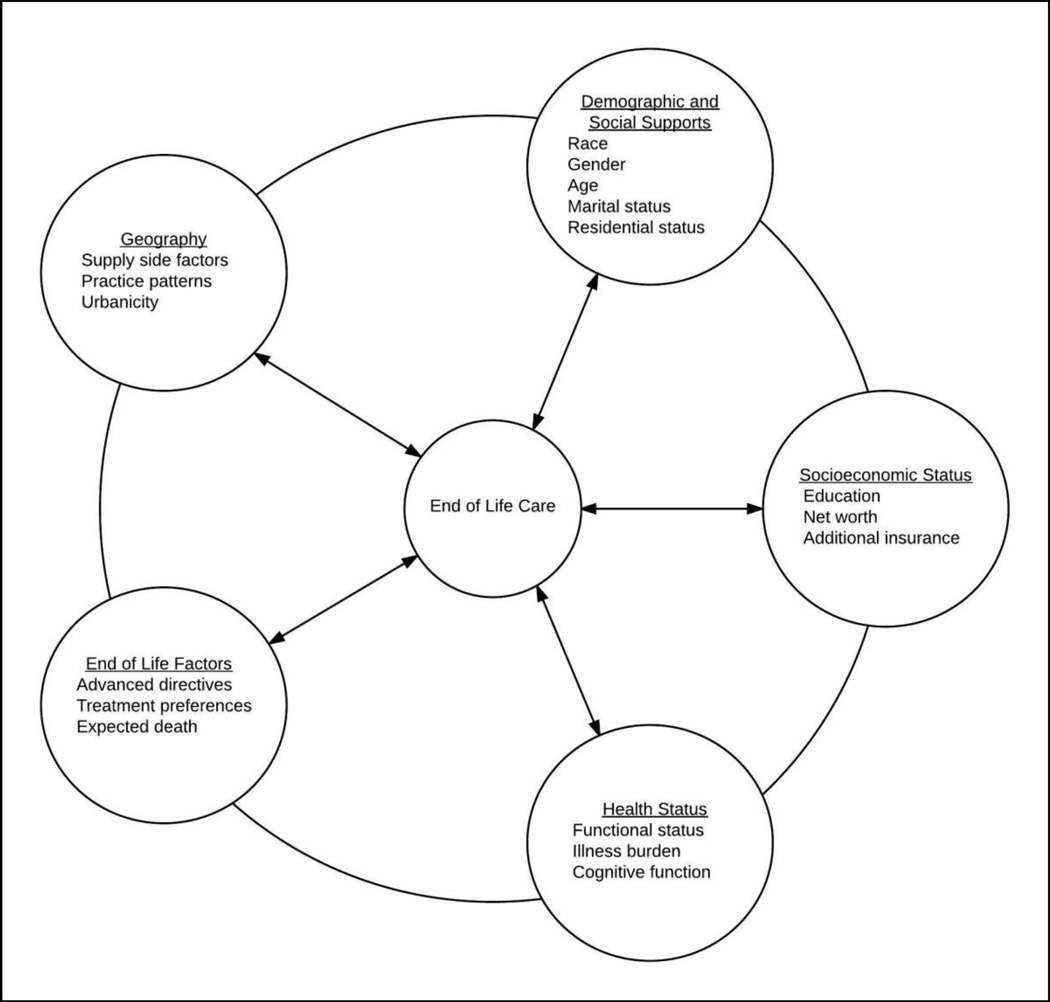
Measurements: Total Medicare expenditures in the last 180 days of life according to race and ethnicity, controlling for demographic factors, social supports, geography, illness burden, and EOL planning factors, including presence of advance directives, discussion of EOL treatment preferences, and whether death had been expected.
Results: The analysis included 5,548 (78.1%) non-Hispanic white, 1,030 (14.5%) non-Hispanic black, and 331 (4.7%) Hispanic adults and 196 (2.8%) adults of other race or ethnicity. Unadjusted results suggest that average EOL Medicare expenditures were $13,522 (35%, P < .001) more for black decedents and $16,341 (42%, P < .001) more for Hispanics than for whites. Controlling for demographic, socioeconomic, geographic, medical, and EOL-specific factors, the Medicare expenditure difference between groups fell to $8,047 (22%, P < .001) more for black and $6,855 (19%, P < .001) more for Hispanic decedents than expenditures for non-Hispanic whites. The expenditure differences between groups remained statistically significant in all models.
Conclusion: Individuals-level factors, including EOL planning factors do not fully explain racial and ethnic differences in Medicare spending in the last 6 months of life. Future research should focus on broader systemic, organizational, and provider-level factors to explain these differences.
Keywords: Medicare; disparities; end-of-life; race and ethnicity.
© 2016, Copyright the Authors Journal compilation © 2016, The American Geriatrics Society.
Conflict of interest statement
Checklist: Elements ofFinancial/PersonalConflicts *Author 1EB Author 2JAH Author 3KML Etc.TJI Yes No Yes No Yes No Yes No Employment or Affiliation x x x x Grants/Funds x x x x Honoraria x x x x Speaker Forum x x x x Consultant x x x x Stocks x x x x Royalties x x x x Expert Testimony x x x x Board Member x x x x Patents x x x x Personal Relationship x x x x output.txt Authors can be listed by abbreviations of their names. For “yes” x mark(s): give brief explanation below: ________________________________________________________ ________________________________________________________
Figures

References
-
- Borum ML, Lynn J, Zhong Z. The effects of patient race on outcomes in seriously ill patients in SUPPORT: an overview of economic impact, medical intervention, and end-of-life decisions. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments. Journal of the American Geriatrics Society. 2000;48(5 Suppl):S194–S198. - PubMed
-
- Hanchate A, Kronman AC, Young-Xu Y, Ash AS, Emanuel E. Racial and ethnic differences in end-of-life costs: why do minorities cost more than whites? Archives of internal medicine. 2009;169(5):493–501. Epub 2009/03/11. doi: 10.1001/archinternmed.2008.616. PubMed PMID: 19273780; PubMed Central PMCID: PMCPMC3621787. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
