

Imaging in Colorectal Cancer: Progress and Challenges for the Clinicians
- PMID: 27589804
- PMCID: PMC5040983
- DOI: 10.3390/cancers8090081
Imaging in Colorectal Cancer: Progress and Challenges for the Clinicians
Abstract
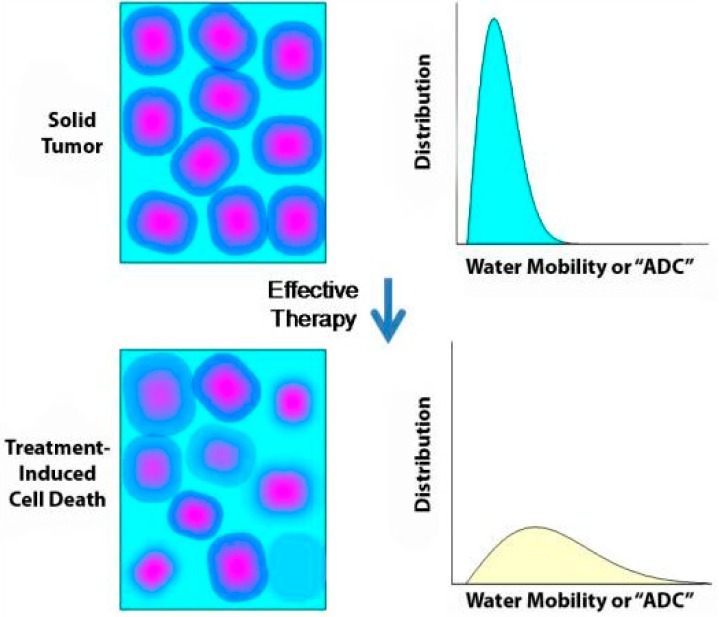
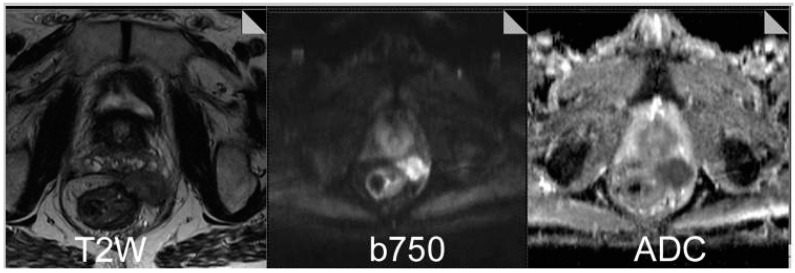
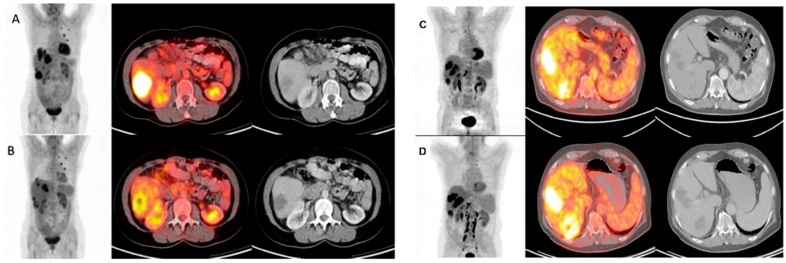
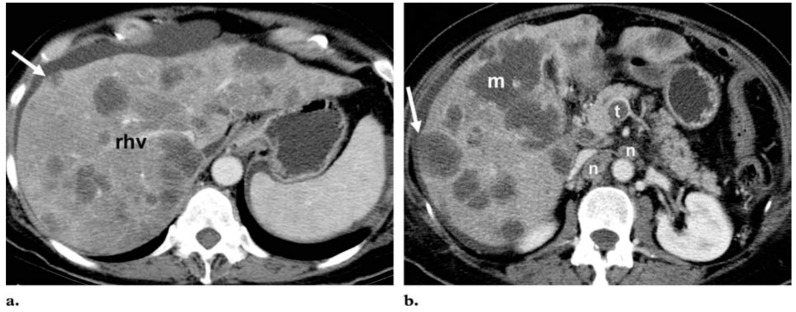
The use of imaging in colorectal cancer (CRC) has significantly evolved over the last twenty years, establishing important roles in surveillance, diagnosis, staging, treatment selection and follow up. The range of modalities has broadened with the development of novel tracer and contrast agents, and the fusion of technologies such as positron emission tomography (PET) and computed tomography (CT). Traditionally, the most widely used modality for assessing treatment response in metastasised colon and rectal tumours is CT, combined with use of the RECIST guidelines. However, a growing body of evidence suggests that tumour size does not always adequately correlate with clinical outcomes. Magnetic resonance imaging (MRI) is a more versatile technique and dynamic contrast-enhanced (DCE)-MRI and diffusion-weighted (DW)-MRI may be used to evaluate biological and functional effects of treatment. Integrated fluorodeoxyglucose (FDG)-PET/CT combines metabolic and anatomical imaging to improve sensitivity and specificity of tumour detection, and a number of studies have demonstrated improved diagnostic accuracy of this modality in a variety of tumour types, including CRC. These developments have enabled the progression of treatment strategies in rectal cancer and improved the detection of hepatic metastatic disease, yet are not without their limitations. These include technical, economical and logistical challenges, along with a lack of robust evidence for standardisation and formal guidance. In order to successfully apply these novel imaging techniques and utilise their benefit to provide truly personalised cancer care, advances need to be clinically realised in a routine and robust manner.
Keywords: angiogenesis; imaging; metastatic colorectal cancer.
Conflict of interest statement
R.G.J. has received honoraria for advisory boards from Roche, Sanofi, Eli Lilley, Amgen and Merck Serono, honoraria for lectures from Roche, Sanofi, and Merck Serono. Financial support to attend international meetings and received funding and free supply of bevacizumab from Roche in a phase II clinical trial. P.F., R.G.H.B.T., H.V. and T.S. have no conflicts of interest.
Figures
References
-
- Globocan F.S. Colorectal Cancer: Estimated Incidence, Mortality and Prevalence Worldwide in 2012. [(accessed on 30 August 2015)]. Available online: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
