

Hospitalization costs for community-acquired pneumonia in Dutch elderly: an observational study
- PMID: 27589847
- PMCID: PMC5010739
- DOI: 10.1186/s12879-016-1783-9
Hospitalization costs for community-acquired pneumonia in Dutch elderly: an observational study
Erratum in
-
Erratum to: Hospitalization costs for community-acquired pneumonia in Dutch elderly: an observational study.BMC Infect Dis. 2016 Nov 24;16(1):702. doi: 10.1186/s12879-016-2015-z. BMC Infect Dis. 2016. PMID: 27884117 Free PMC article. No abstract available.
Abstract
Background: Community-acquired pneumonia (CAP) is one of the most common infections, especially in the elderly (≥65 years). The aim of this study was to quantify hospitalization costs for CAP in different age groups and in patients with different CAP risk profiles. Secondary objectives were to assess disease severity differences between placebo and vaccine receiving participants and identify cost driving factors of CAP in hospitalized elderly in the Netherlands.
Methods: This prospective cohort study of hospitalized CAP patients was executed in parallel to the Community Acquired Pneumonia Immunization Trial in Adults (CAPiTA). Within the CAPiTA, a cohort of 84,496 subjects aged ≥65, all suspected CAP-episodes presenting in one of the 58 participating hospitals between September 2008 and August 2013 were included. CAP was diagnosed on clinical and radiographical criteria. Invasive pneumococcal disease (IPD) and non-IPD-CAP episodes, regardless of the causing pathogen, were evaluated separately. Costs were calculated by multiplying recorded healthcare resources with Dutch unit cost prices for the year 2012. Multivariate regression analysis was performed to identify cost drivers.
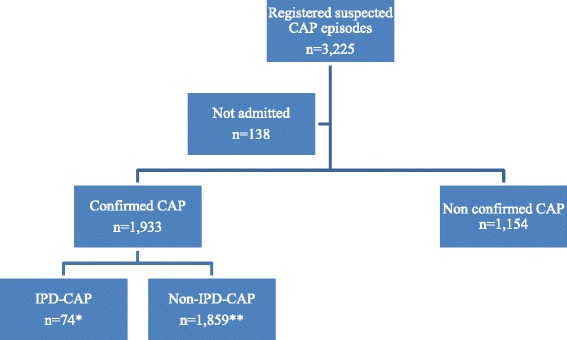
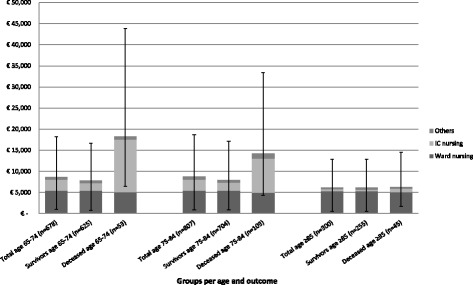
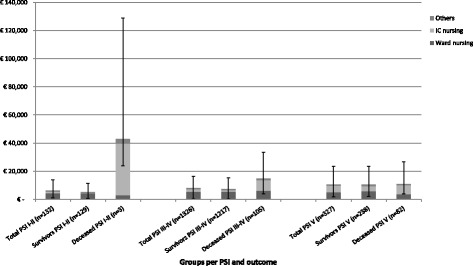
Results: In the sentinel hospitals 3225 suspected CAP and IPD episodes were included, of which 1933 were radiographically confirmed by chest X-ray. Analyses were conducted on confirmed CAP episodes only. Overall mean length of hospital stay was 12.1 days, the in-hospital mortality rate was 11.26 %, and mean costs were €8301 (95 % CI: €7760-€8999). When stratified in age-categories 65-74, 75-84 and ≥85, mean hospitalization costs were €8674, €8770 and €6197, respectively (p = 0.649). IPD-CAP and non-IPD-CAP mean hospitalization costs were €13,611 and €8081, respectively. Higher CURB-65 score and individuals at medium risk for developing pneumococcal disease were significantly associated with higher costs. Being male, lower age, previous admissions, lower risk, lower urbanity and higher socio-economic status were associated with lower costs.
Conclusions: Mean hospitalization costs of a CAP subject were €8301 and higher for IPD-CAP compared to non-IPD-CAP cases. Medium risk patients and higher CURB-65 scores were identified as cost driving factors.
Keywords: Community-acquired pneumonia; Costing study; Elderly; Hospitalization; Invasive pneumococcal disease; Risk-groups.
Figures
References
-
- Oosterheert JJ, Bonten MJ, Hak E, Lammers JW, Schneider MM, Hoepelman IM. The increase in pneumonia-related morbidity and mortality among adults in the Netherlands and possible explanations for it. Ned Tijdschr Geneeskd. 2004;148(36):1765–1769. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
