

Effect of a Home-Based Palliative Care Program on Healthcare Use and Costs
- PMID: 27590922
- PMCID: PMC5118096
- DOI: 10.1111/jgs.14354
Effect of a Home-Based Palliative Care Program on Healthcare Use and Costs
Abstract
Objectives: To evaluate the nonclinical outcomes of a proactive palliative care program funded and operated by a health system for Medicare Advantage plan beneficiaries.
Design: Observational, retrospective study using propensity-based matching.
Setting: A health system in southern California.
Participants: Individuals who received the intervention between 2007 and 2014 (n = 368) were matched with 1,075 comparison individuals within each of four disease groups: cancer, chronic obstructive pulmonary disease, heart failure, and dementia. All were known to be dead at the time of the retrospective study, were Medicare Advantage beneficiaries, and had 2 years of usage data before death. Median age at death for each disease group was older than 80.
Intervention: Home- and clinic-based palliative care (PC) services provided by a multidisciplinary team.
Measurements: Outcomes included hospital costs, other healthcare costs, readmission rates, hospital admissions and bed days, intensive care unit use in final 30 days of life, and death within 30 days of an admission.
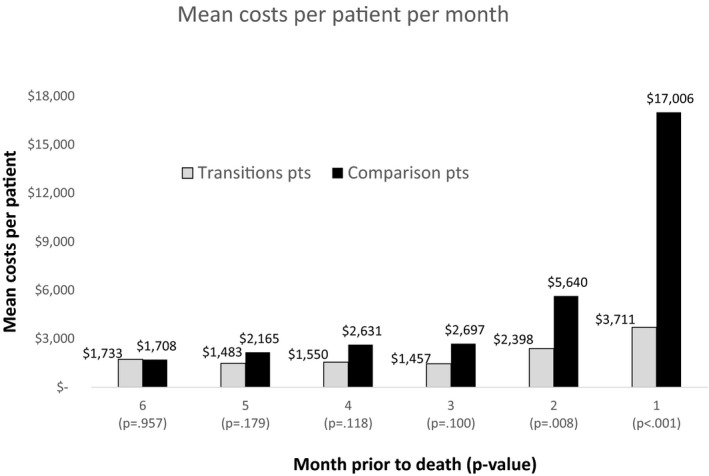
Results: Intervention participants in all four disease groups had less hospital use and lower hospital costs nonintervention participants, which drove lower overall healthcare costs. In the final 6 months of life, healthcare costs for the intervention groups stayed largely the same from month to month, whereas costs for comparison participants increased dramatically.
Conclusion: In the context of an alternative payment model in which the provider was "at risk" of bearing the costs of care, a proactive PC program helped to avoid the escalation in hospital use and costs commonly seen in the final months of life.
Keywords: Medicare Advantage; costs; palliative care; serious illness; utilization.
© 2016 The Authors. The Journal of the American Geriatrics Society published by Wiley Periodicals, Inc. on behalf of The American Geriatrics Society.
Figures
References
-
- Rabow MW, Smith AK, Braun JL et al. Outpatient palliative care practices. Arch Intern Med 2010;170:654–655. - PubMed
-
- Rabow M, Kvale E, Barbour L et al. Moving upstream: A review of the evidence of the impact of outpatient palliative care. J Palliat Med 2013;16:1540–1549. - PubMed
-
- Teno JM, Clarridge BR, Casey V et al. Family perspectives on end‐of‐life care at the last place of care. JAMA 2004;291:88–93. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
