

Preoperative risk factors for conversion from laparoscopic to open cholecystectomy: a validated risk score derived from a prospective U.K. database of 8820 patients
- PMID: 27591176
- PMCID: PMC5094477
- DOI: 10.1016/j.hpb.2016.07.015
Preoperative risk factors for conversion from laparoscopic to open cholecystectomy: a validated risk score derived from a prospective U.K. database of 8820 patients
Abstract
Background: Laparoscopic cholecystectomy is commonly performed, and several factors increase the risk of open conversion, prolonging operating time and hospital stay. Preoperative stratification would improve consent, scheduling and identify appropriate training cases. The aim of this study was to develop a validated risk score for conversion for use in clinical practice.
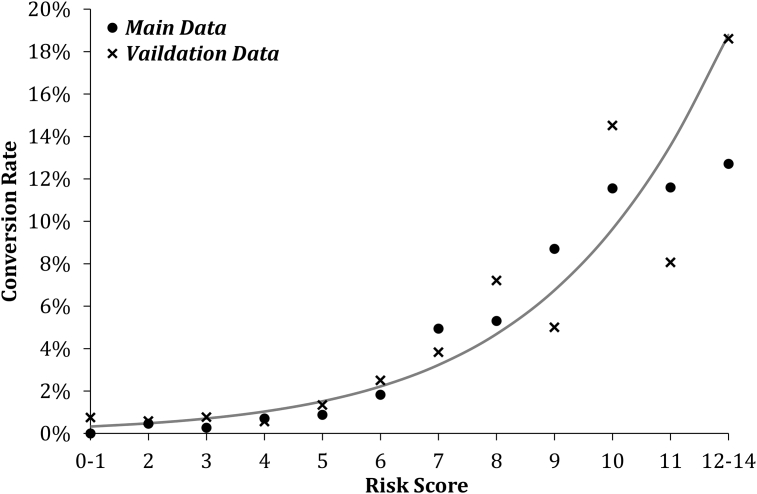
Patients and methods: Preoperative patient and disease-related variables were identified from a prospective cholecystectomy database (CholeS) of 8820 patients, divided into main and validation sets. Preoperative predictors of conversion were identified by multivariable binary logistic regression. A risk score was developed and validated using a forward stepwise approach.
Results: Some 297 procedures (3.4%) were converted. The risk score was derived from six significant predictors: age (p = 0.005), sex (p < 0.001), indication for surgery (p < 0.001), ASA (p < 0.001), thick-walled gallbladder (p = 0.040) and CBD diameter (p = 0.004). Testing the score on the validation set yielded an AUROC = 0.766 (p < 0.001), and a score >6 identified patients at high risk of conversion (7.1% vs. 1.2%).
Conclusion: This validated risk score allows preoperative identification of patients at six-fold increased risk of conversion to open cholecystectomy.
Copyright © 2016 International Hepato-Pancreato-Biliary Association Inc. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Goonawardena J., Gunnarsson R., de Costa A. Predicting conversion from laparoscopic to open cholecystectomy presented as a probability nomogram based on preoperative patient risk factors. Am J Surg. 2015;210:492–500. - PubMed
-
- Rosen M., Brody F., Ponsky J. Predictive factors for conversion of laparoscopic cholecystectomy. Am J Surg. 2002;184:254–258. - PubMed
-
- Lipman J.M., Claridge J.A., Haridas M., Martin M.D., Yao D.C., Grimes K.L. Preoperative findings predict conversion from laparoscopic to open cholecystectomy. Surgery. 2007;142:556–563. - PubMed
-
- Ballal M., David G., Willmott S., Corless D.J., Deakin M., Slavin J.P. Conversion after laparoscopic cholecystectomy in England. Surg Endosc. 2009;23:2338–2344. - PubMed
-
- Strasberg S.M., Hertl M., Soper N.J. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995;180:101–125. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
