

Echocardiography as a guide for fluid management
- PMID: 27592289
- PMCID: PMC5010858
- DOI: 10.1186/s13054-016-1407-1
Echocardiography as a guide for fluid management
Abstract
Background: In critically ill patients at risk for organ failure, the administration of intravenous fluids has equal chances of resulting in benefit or harm. While the intent of intravenous fluid is to increase cardiac output and oxygen delivery, unwelcome results in those patients who do not increase their cardiac output are tissue edema, hypoxemia, and excess mortality. Here we briefly review bedside methods to assess fluid responsiveness, focusing upon the strengths and pitfalls of echocardiography in spontaneously breathing mechanically ventilated patients as a means to guide fluid management. We also provide new data to help clinicians anticipate bedside echocardiography findings in vasopressor-dependent, volume-resuscitated patients.
Objective: To review bedside ultrasound as a method to judge whether additional intravenous fluid will increase cardiac output. Special emphasis is placed on the respiratory effort of the patient.
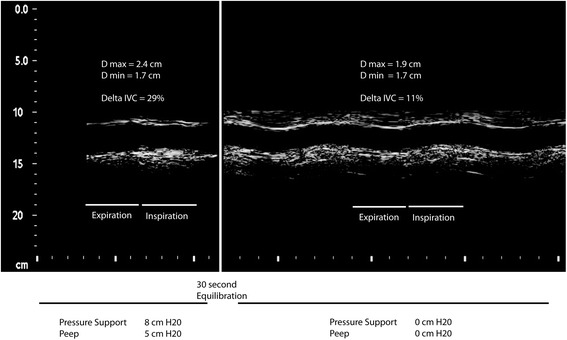
Conclusions: Point-of-care echocardiography has the unique ability to screen for unexpected structural findings while providing a quantifiable probability of a patient's cardiovascular response to fluids. Measuring changes in stroke volume in response to either passive leg raising or changes in thoracic pressure during controlled mechanical ventilation offer good performance characteristics but may be limited by operator skill, arrhythmia, and open lung ventilation strategies. Measuring changes in vena caval diameter induced by controlled mechanical ventilation demands less training of the operator and performs well during arrythmia. In modern delivery of critical care, however, most patients are nursed awake, even during mechanical ventilation. In patients making respiratory efforts we suggest that ventilator settings must be standardized before assessing this promising technology as a guide for fluid management.
Keywords: Echocardiography; Point-of-care ultrasound; Resuscitation; Shock.
Figures
References
-
- Sarnoff SJ. Myocardial contractility as described by ventricular function curves; observations on Starling’s law of the heart. Physiol Rev. 1955;35:107–22. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
