

Hypoalbuminemia, Low Base Excess Values, and Tachypnea Predict 28-Day Mortality in Severe Sepsis and Septic Shock Patients in the Emergency Department
- PMID: 27593863
- PMCID: PMC5011267
- DOI: 10.3349/ymj.2016.57.6.1361
Hypoalbuminemia, Low Base Excess Values, and Tachypnea Predict 28-Day Mortality in Severe Sepsis and Septic Shock Patients in the Emergency Department
Abstract
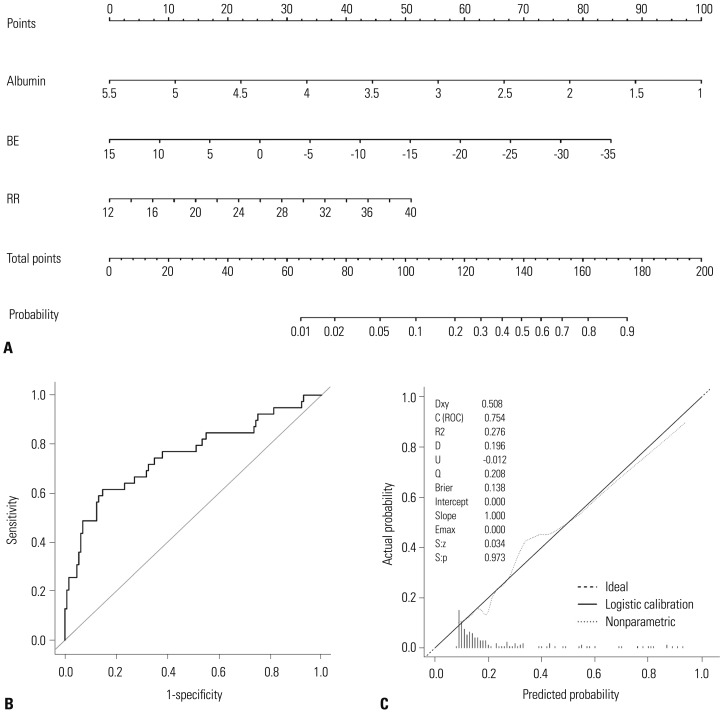
Purpose: The objective of this study was to develop a new nomogram that can predict 28-day mortality in severe sepsis and/or septic shock patients using a combination of several biomarkers that are inexpensive and readily available in most emergency departments, with and without scoring systems.
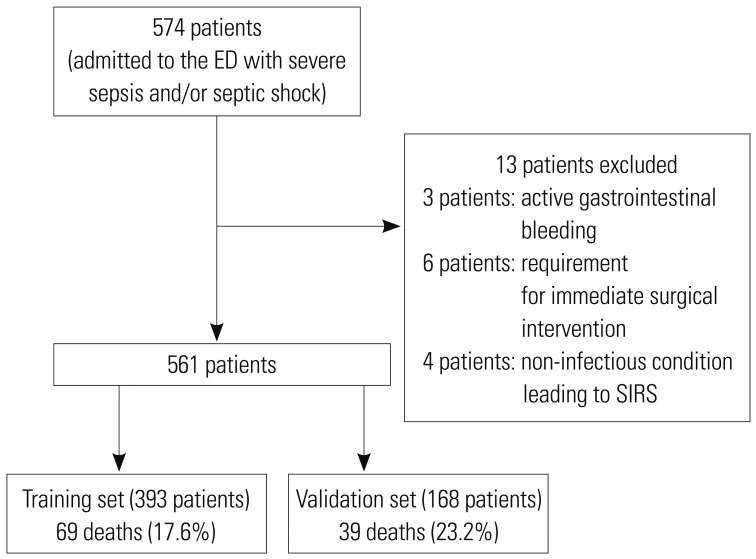
Materials and methods: We enrolled 561 patients who were admitted to an emergency department (ED) and received early goal-directed therapy for severe sepsis or septic shock. We collected demographic data, initial vital signs, and laboratory data sampled at the time of ED admission. Patients were randomly assigned to a training set or validation set. For the training set, we generated models using independent variables associated with 28-day mortality by multivariate analysis, and developed a new nomogram for the prediction of 28-day mortality. Thereafter, the diagnostic accuracy of the nomogram was tested using the validation set.
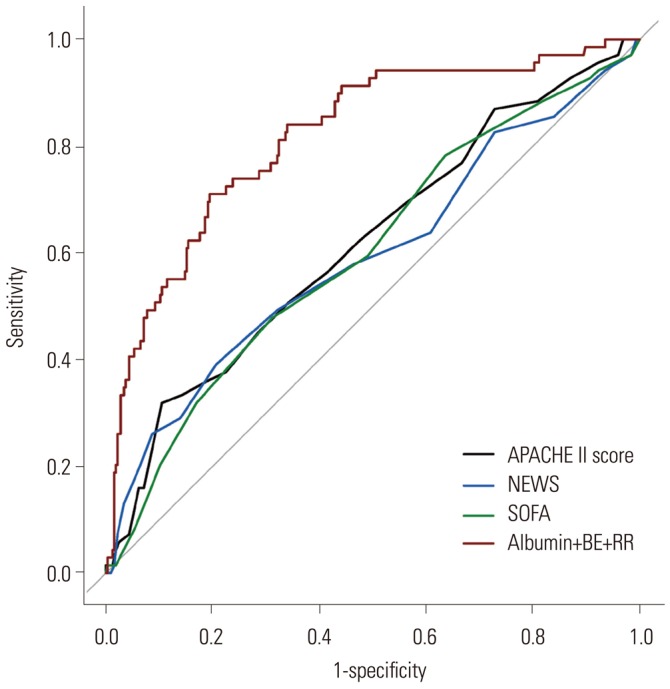
Results: The prediction model that included albumin, base excess, and respiratory rate demonstrated the largest area under the receiver operating characteristic curve (AUC) value of 0.8173 [95% confidence interval (CI), 0.7605-0.8741]. The logistic analysis revealed that a conventional scoring system was not associated with 28-day mortality. In the validation set, the discrimination of a newly developed nomogram was also good, with an AUC value of 0.7537 (95% CI, 0.6563-0.8512).
Conclusion: Our new nomogram is valuable in predicting the 28-day mortality of patients with severe sepsis and/or septic shock in the emergency department. Moreover, our readily available nomogram is superior to conventional scoring systems in predicting mortality.
Keywords: Severe sepsis; mortality; nomograms; septic shock.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Angus DC, van der Poll T. Severe sepsis and septic shock. N Engl J Med. 2013;369:840–851. - PubMed
-
- Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012. JAMA. 2014;311:1308–1316. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–1554. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
