

A Case of Pulmonary Interstitial Emphysema Treated by Percutaneous Catheter Insertion in Extremely Low Birth Weight Infant
- PMID: 27593885
- PMCID: PMC5011289
- DOI: 10.3349/ymj.2016.57.6.1523
A Case of Pulmonary Interstitial Emphysema Treated by Percutaneous Catheter Insertion in Extremely Low Birth Weight Infant
Abstract
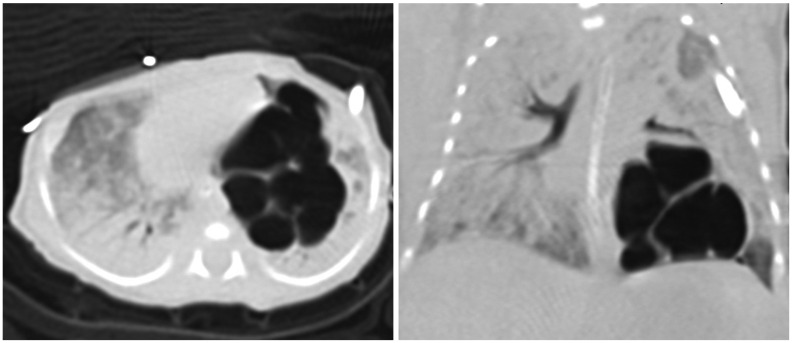
The pulmonary interstitial emphysema (PIE) is a life-threatening illness in premature infants with mechanical ventilation. While most are managed conservatively, decompression would be necessary. Here, we report the first case of PIE treated by percutaneous catheter insertion in an extremely low birth weight (ELBW) infant in Korea. The patient, born with 660 g in 23+2 weeks of gestation, showed PIE in left lower lung on postnatal day 12. Percutaneous catheter insertion was performed on postnatal day 25. The size of PIE decreased, but didn't disappear completely. On postnatal day 42, we exchanged catheter and inserted additional catheter in pleural space. However, sudden desaturation and pneumothorax occurred on postnatal day 44. We changed catheter in pleural space, and pneumothorax and PIE improved. Finally, we successfully removed catheters, and weaned patient out. As in our case, percutaneous catheter insertion would be a useful option for ELBW infants with PIE.
Keywords: Pulmonary emphysema; catheters, indwelling; extremely low birth weight infant; premature infant.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures

Similar articles
-
Pulmonary interstitial emphysema after resolution of relapsing pneumothorax and discontinuation of mechanical ventilation. An atypical case in a preterm infant.J Matern Fetal Neonatal Med. 2014 Oct;27(15):1610-2. doi: 10.3109/14767058.2013.867322. Epub 2013 Dec 16. J Matern Fetal Neonatal Med. 2014. PMID: 24245490
-
Unilateral neonatal pulmonary interstitial emphysema managed conservatively: A case report.Pediatr Pulmonol. 2021 Jan;56(1):83-87. doi: 10.1002/ppul.25112. Epub 2020 Oct 20. Pediatr Pulmonol. 2021. PMID: 33080119
-
Percutaneous catheter evacuation of a pneumatocele in an extremely premature infant with respiratory failure.J Perinatol. 2003 Sep;23(6):516-8. doi: 10.1038/sj.jp.7210964. J Perinatol. 2003. PMID: 13679944
-
Challenging acquired pulmonary interstitial emphysema in an extreme preterm infant: A case report and review of literature.J Neonatal Perinatal Med. 2024 Nov;17(6):863-868. doi: 10.1177/19345798241296332. Epub 2024 Nov 8. J Neonatal Perinatal Med. 2024. PMID: 40016986 Review.
-
CT imaging of pulmonary lobar interstitial emphysema in a spontaneous breathing preterm infant.Am J Perinatol. 2002 Aug;19(6):285-90. doi: 10.1055/s-2002-34466. Am J Perinatol. 2002. PMID: 12357418 Review.
Cited by
-
Case Report: Neurally adjusted ventilatory assist as an effective rescue treatment for pulmonary interstitial emphysema in extremely low birth weight infants.Front Pediatr. 2024 Jan 22;12:1332332. doi: 10.3389/fped.2024.1332332. eCollection 2024. Front Pediatr. 2024. PMID: 38318454 Free PMC article.
-
Percutaneous Drainage for Giant Pulmonary Interstitial Emphysema in a Tiny Infant with a Birth Weight of 327 g.AJP Rep. 2024 May 3;14(2):e133-e135. doi: 10.1055/s-0044-1786713. eCollection 2024 Apr. AJP Rep. 2024. PMID: 38707264 Free PMC article.
References
-
- Morisot C, Kacet N, Bouchez MC, Rouland V, Dubos JP, Gremillet C, et al. Risk factors for fatal pulmonary interstitial emphysema in neonates. Eur J Pediatr. 1990;149:493–495. - PubMed
-
- Jassal MS, Benson JE, Mogayzel PJ., Jr Spontaneous resolution of diffuse persistent pulmonary interstitial emphysema. Pediatr Pulmonol. 2008;43:615–619. - PubMed
-
- Jeng MJ, Lee YS, Tsao PC, Soong WJ. Neonatal air leak syndrome and the role of high-frequency ventilation in its prevention. J Chin Med Assoc. 2012;75:551–559. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
