

Comparison of 1869 thyroid ultrasound-guided fine-needle aspiration biopsies between general surgeons and interventional radiologists
- PMID: 27594994
- PMCID: PMC4995479
- DOI: 10.1016/j.amsu.2016.07.015
Comparison of 1869 thyroid ultrasound-guided fine-needle aspiration biopsies between general surgeons and interventional radiologists
Abstract
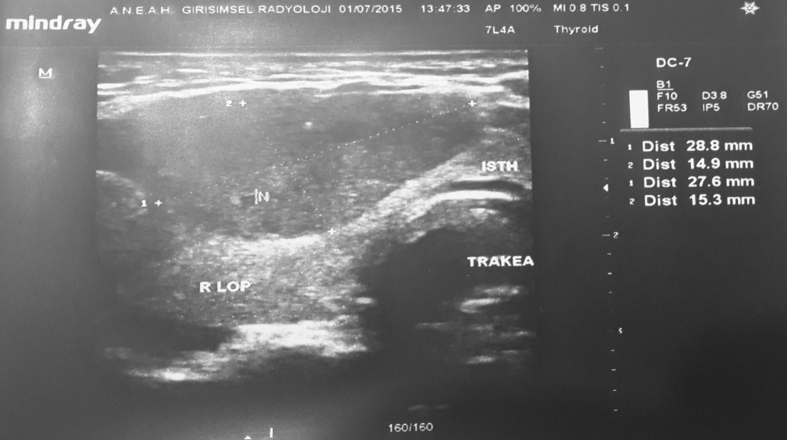
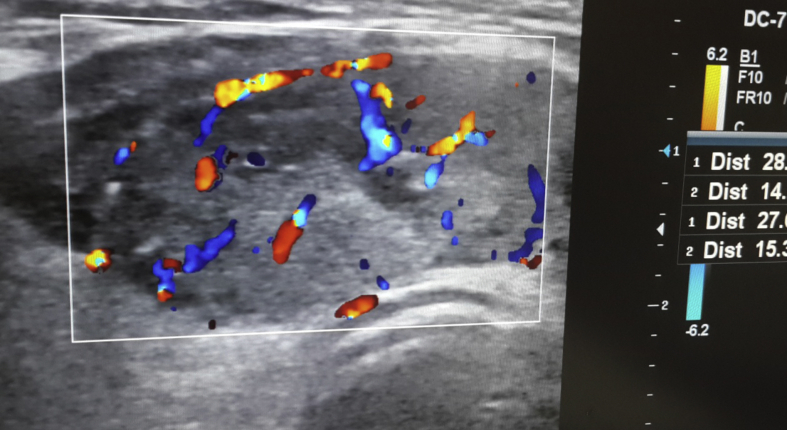
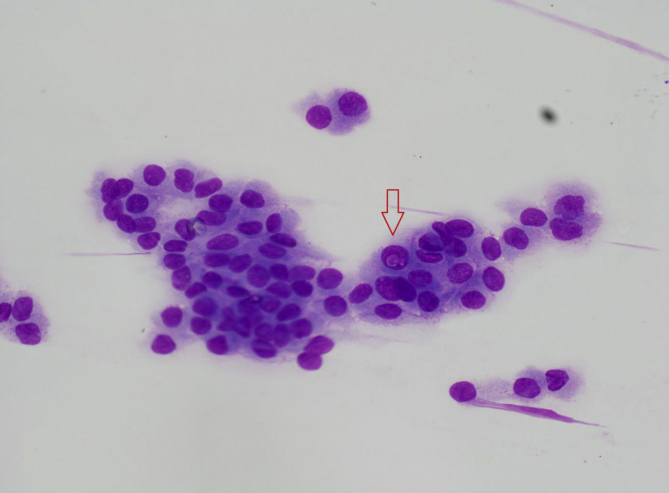
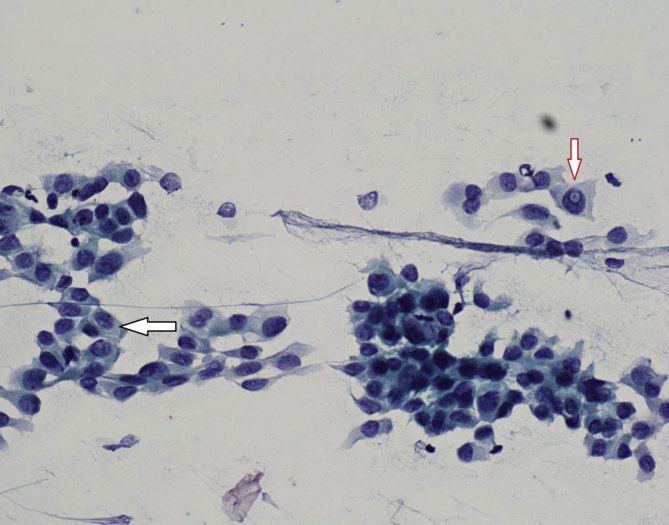
Background: Thyroid nodules are commonly encountered problems in clinical practice. For patients who have a thyroid nodule, the fine-needle aspiration biopsy (FNAB) is the most important test, as it is the most reliable diagnostic method for distinguishing between benign thyroid nodules and cancerous nodules. FNAB is able to be performed either via an ultrasound (USG) or alone and is the first choice when it comes to diagnosing thyroid nodules, given that it is cheap, safe and provides accurate results.
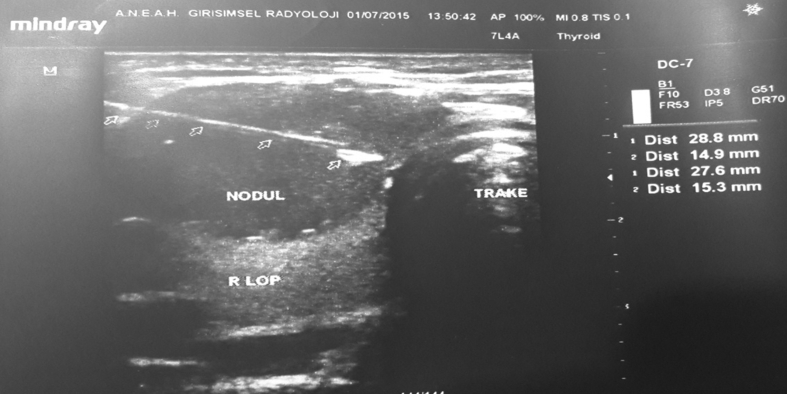
Objective: In this study-a retrospective analysis of FNAB via USG - our aim is to evaluate the multiple variables related to FNAB procedures, including the experience of the person performing the biopsy, the age and gender of the patient, the number of nodules, the size of the nodule(s) and the number of lams recorded from the cytopathology report on non-diagnostic rates, conducted at an invasive radiology clinic and at a general surgery clinic.
Materials and methods: A total of 1062 patients involving 1869 nodules, examined using FNAB via USG, were reviewed retrospectively from records dated between November 2011 and July 2014 and from pathology reports taken from the ANEAH General Surgery clinic and Interventional Radiology clinic. Cytopathology results were classified according to the 2007 Bethesda System for Reporting. Gender, age, number of nodules, diameter of the nodules, biopsied nodules, location of the nodules, number of lams, symptoms and the date of biopsies were the parameters used to examine the factors involved in non-diagnostic cytopathology invasive radiology. These parameters were inspected at both of the clinics (ANEAH General Surgery clinic and Interventional Radiology clinic). In analyzing the results, the statistical significance level was set at 0.05, where in cases that the p value was under 0.05 (p < 0.05), it was determined that no significant relationship existed. In this study, data were analyzed using SPSS 20 software.
Results: Of the nodules reviewed, 1620 were found on females and 249 on males. The age of the patients ranged from 10 to 87 years, with the mean age being 50 years. In the general surgery clinic, 470 nodules of 341 patients were aspirated, and in the interventional radiological clinic, 1399 nodules of 721 patients were aspirated. In the literature review conducted to compare statistical assessments of FNAB via USG, no significant difference was found between the ANEAH General Surgery clinic and the Invasive Radiology clinic (p > 0.05). In the invasive radiology clinic, non-diagnostic rates decreased with the increase in experience of the person who conducted the biopsy (p = 0.001).
Conclusion: The results from both of the clinic's rates of non-diagnostic FNAB, performed via USG, were found to be acceptable. Our study also demonstrates that USG-guided FNAB can be performed with a low non-diagnostic rate as experience grows.
Keywords: FNAB; Non-diagnostic; Thyroid USG; Thyroid biopsy.
Figures

References
-
- Revised American thyroid association management guidelines for patients with thyroid nodules and differentiated thyroid Cancer the American thyroid association (ATA) guidelines taskforce on thyroid nodules and differentiated thyroid. Cancer Thyroid. 2009;19:1167–1214. - PubMed
-
- Lal G., Clark O.H. Thyroid and parathyroid. In: Brunicardi F.C., Schwartz S.I., editors. Schwartz's Principle of Surgery. 9 th Ed. Mc Graw Hill; New York: 2010. pp. 1344–1373.
-
- Morgan J.L., Serpell J.W., Cheng M.S. Fine needle aspiration cytolgy of throid nodüles: how useful is it? Aust. N. Z. J. Surg. 2003;73:480. - PubMed
-
- Theoharis C.G., Schofield K.M., Hammers L., Udelsman R., Chhieng D.C. The Bethesda thyroid fine-needle aspiration classification system: year 1 at an academic institution. Thyroid. 2009;19(11):1215–1223. - PubMed
-
- Nguyen G.K., Ginsberg J., Crockford P.M. Fine-needle aspiration biopsy cytology of the thyroid. Its value and limitations in the diagnosis and management of solitary thyroid nodules. Pathol. Annu. 1991;26:63–69. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
