

doi: 10.1038/nm.4161.
Epub 2016 Sep 5.
Characterization of progressive HIV-associated tuberculosis using 2-deoxy-2-[18F]fluoro-D-glucose positron emission and computed tomography
Affiliations
- PMID: 27595321
- PMCID: PMC5055809
- DOI: 10.1038/nm.4161
Item in Clipboard
Characterization of progressive HIV-associated tuberculosis using 2-deoxy-2-[18F]fluoro-D-glucose positron emission and computed tomography
Nat Med.
2016 Oct.
Abstract
Tuberculosis is classically divided into states of latent infection and active disease. Using combined positron emission and computed tomography in 35 asymptomatic, antiretroviral-therapy-naive, HIV-1-infected adults with latent tuberculosis, we identified ten individuals with pulmonary abnormalities suggestive of subclinical, active disease who were substantially more likely to progress to clinical disease. Our findings challenge the conventional two-state paradigm and may aid future identification of biomarkers that are predictive of progression.
Conflict of interest statement
statements The authors declare no competing financial interests
Figures
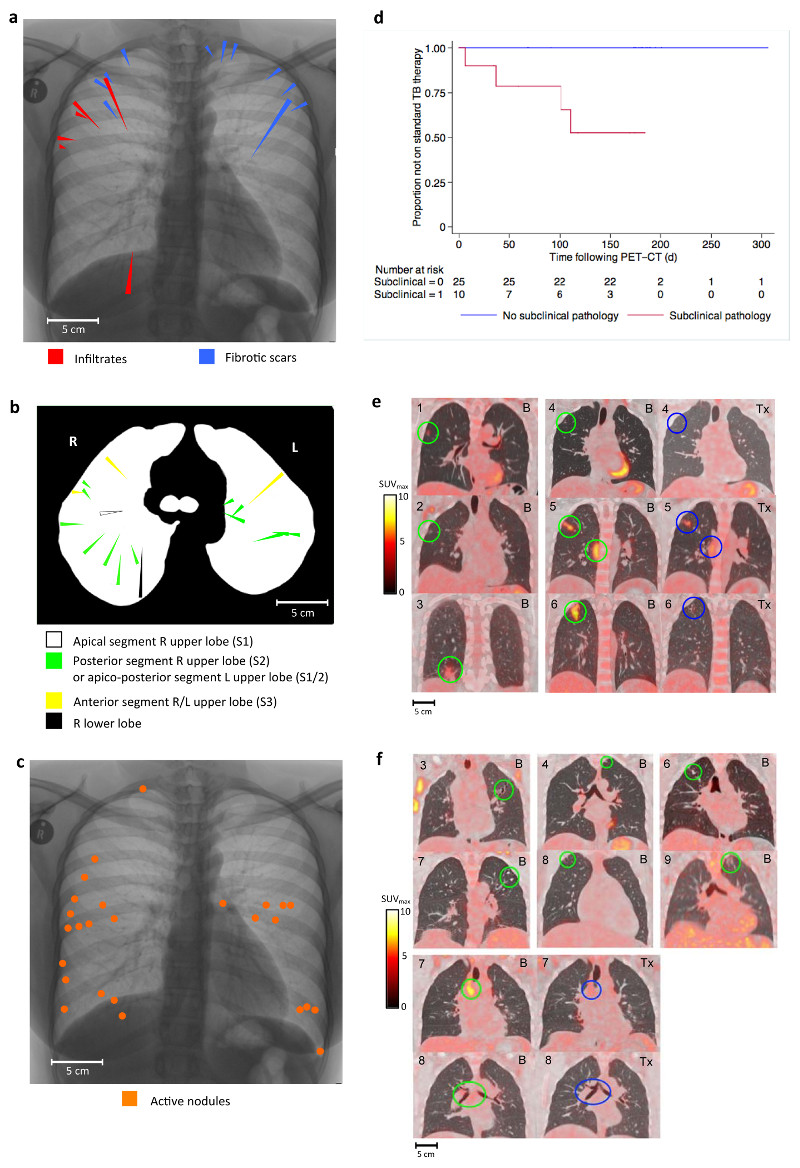
a – Spatial overview of the FDG-PET/CT location of six infiltrates and 12 scars identified in nine participants in coronal plane. Lesions are represented on a single inverted CXR as triangles. Length of triangle is proportional to length of lesion. b – Spatial overview of the FDG-PET/CT location of 18 infiltrates and scars in nine participants in the axial plane with broncho-pulmonary segment indicated. c – Spatial overview of the FDG-PET/CT location of 26 active nodules found in one participant d – Survival curve showing time to commencing standard 2HRZE/4HR for those with evidence of subclinical pathology (n = 10) and those without (n = 25), P = 0.0003 – log-rank test for equality) e– Lesions from each of the six participants with infiltrates shown on fused FDG-PET/CT images in coronal plane. Participants uniquely numbered 1 – 6 in top left of image. Baseline scans denoted by “B” in top right corner with baseline lesions circled in green. Follow-up scans denoted by “Tx” in top right corner of image with lesions post-treatment circled in blue. For participants “4”, “5” and “6” the treatment received between scans was IPT, 2HRZE and 2HRZE/4HR respectively f – Lesions from each of the six participants with scars (at least one example from each participant). Three participants numbered “3”, “4” and “6” also have infiltrates corresponding to Figure 1e. Lesions in baseline PET/CT scan circled in green. Mediastinal lymph nodes pre and post IPT circled green and blue respectively for participants “7” and “8”.
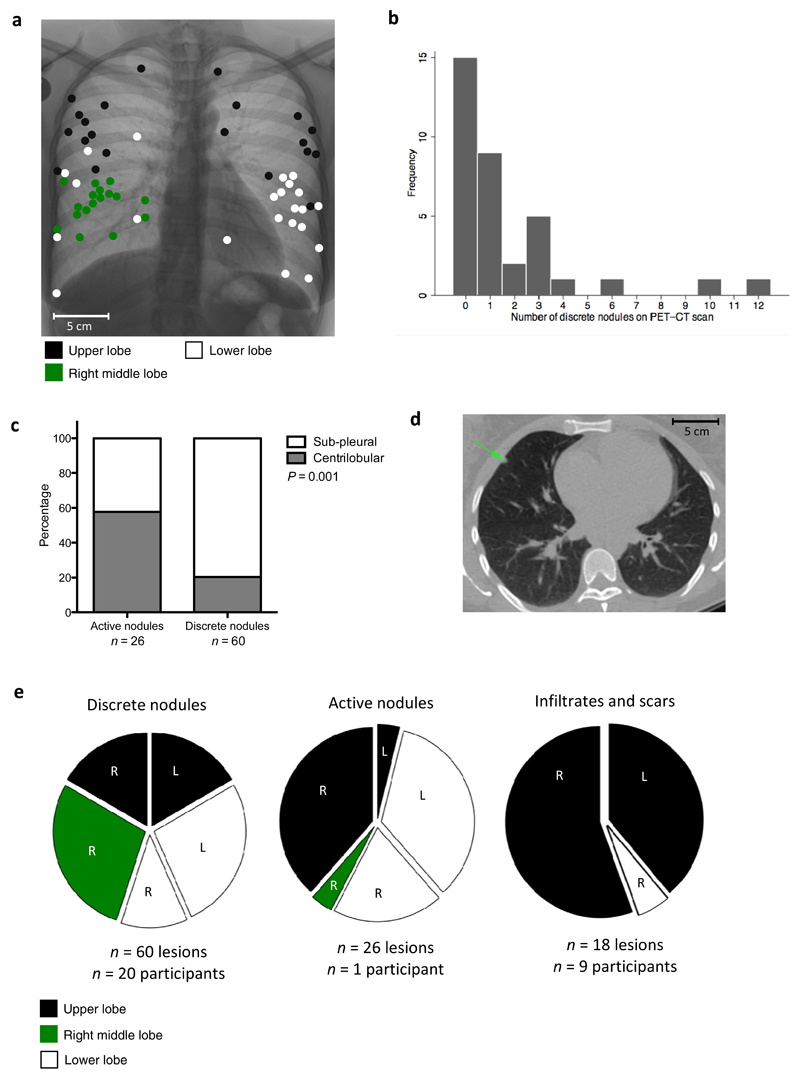
a – Spatial overview of the FDG-PET/CT location of 60 discrete nodules in 20 participants (15 of which did not have other types of lesions) in the coronal plane. Lesions are represented as filled circles with colour denoting lobar location. b – Frequency distribution showing number of discrete nodules found in lung parenchyma per participant. c – Graph showing differences in lobular distribution of discrete compared to active nodules. Discrete nodules are significantly more likely to have a sub-pleural rather than centrilobular location, P = 0.001 - χ2 test. d – Example of a discrete nodule identified with green arrow on an axial section through CT scan. e – Pie chart showing lobar distribution of discrete nodules, active nodules and infiltrates/scars.
Comment in
-
A broader spectrum of tuberculosis.Nat Med. 2016 Oct 6;22(10):1076-1077. doi: 10.1038/nm.4186. Nat Med. 2016. PMID: 27711059 No abstract available.
References
-
- Medlar EM. The pathogenesis of minimal pulmonary tuberculosis; a study of 1,225 necropsies in cases of sudden and unexpected death. Am Rev Tuberc. 1948;58:583–611. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
