

The MEssaging for Diabetes Intervention Reduced Barriers to Medication Adherence Among Low-Income, Diverse Adults With Type 2
- PMID: 27595710
- PMCID: PMC5375078
- DOI: 10.1177/1932296816668374
The MEssaging for Diabetes Intervention Reduced Barriers to Medication Adherence Among Low-Income, Diverse Adults With Type 2
Abstract
Background: Nonadherence to diabetes medication is prevalent and costly. MEssaging for Diabetes (MED), a mobile health (mHealth) intervention, identified and addressed user-specific barriers to medication adherence. We assessed whether MED reduced users' targeted barriers and if barrier reductions were associated with within-participant improvements in adherence or glycemic control (HbA1c).
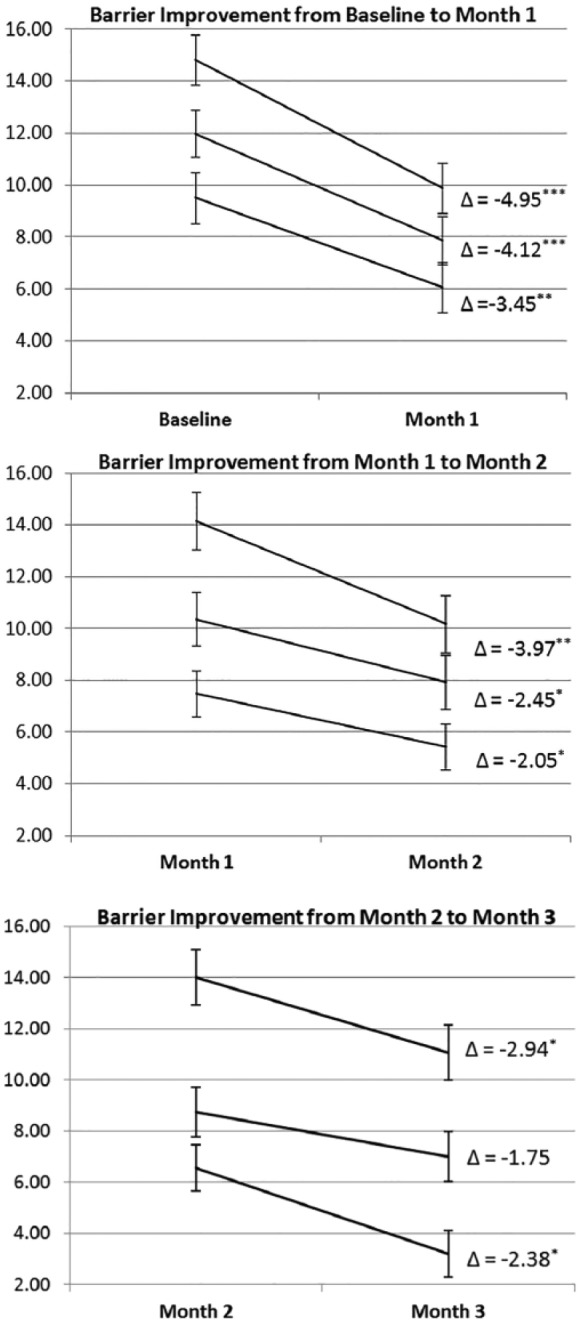
Methods: Adults (N = 80) with type 2 diabetes completed self-report measures identifying barriers to adherence at baseline and monthly for 3 months. At each assessment, 17 barriers were assessed and ranked for each user. Each subsequent month, users received daily text messages addressing their 3 highest ranked barriers. Targeted barriers were different for each participant and could change monthly. Paired t-tests assessed within-participant improvement in targeted barriers each month, and nested regression models assessed if changes in a participant's barrier scores were associated with improvements in adherence and HbA1c.
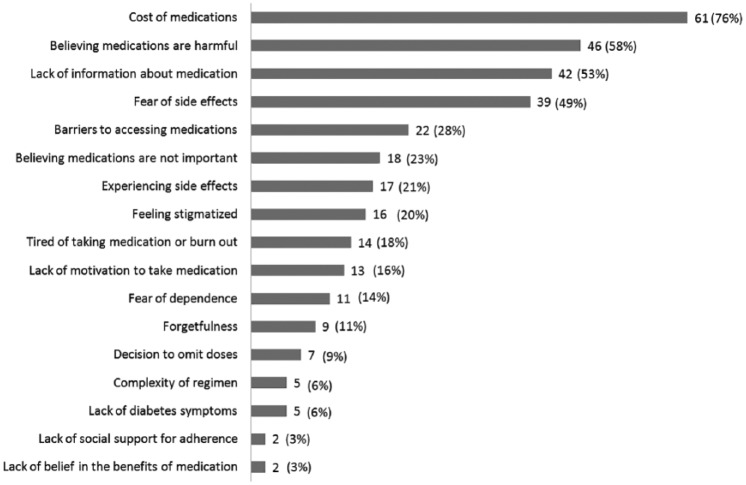
Results: Participants were 69% non-white and 82% had incomes <$25K. Average HbA1c was 8.2 ± 2.0%. Assessment completion rates were 100% at baseline, 59% at 1 month, 30% at 2 months, and 65% at 3 months. The most commonly reported barriers were the cost of medications (76%), believing medications are harmful (58%), and lacking information about medications (53%). Participants' barrier scores improved each month and barrier improvement predicted adherence assessed via nightly adherence assessment text messages ( P < .001). Among participants who completed assessments each month, barrier improvement in months 2 and 3 ( P < .05) predicted HbA1c improvement.
Conclusions: Iterative, individual tailoring may overcome users' barriers to adherence. Attrition is a challenge for mHealth interventions among low-income patients.
Keywords: intervention; mHealth; medication adherence; mobile phone; text message; type 2 diabetes.
Conflict of interest statement
Figures
Similar articles
-
User Engagement Among Diverse Adults in a 12-Month Text Message-Delivered Diabetes Support Intervention: Results from a Randomized Controlled Trial.JMIR Mhealth Uhealth. 2020 Jul 21;8(7):e17534. doi: 10.2196/17534. JMIR Mhealth Uhealth. 2020. PMID: 32706738 Free PMC article. Clinical Trial.
-
mHealth Intervention Elements and User Characteristics Determine Utility: A Mixed-Methods Analysis.Diabetes Technol Ther. 2017 Jan;19(1):9-17. doi: 10.1089/dia.2016.0294. Diabetes Technol Ther. 2017. PMID: 28099052 Free PMC article.
-
Trial to examine text message-based mHealth in emergency department patients with diabetes (TExT-MED): a randomized controlled trial.Ann Emerg Med. 2014 Jun;63(6):745-54.e6. doi: 10.1016/j.annemergmed.2013.10.012. Epub 2013 Nov 11. Ann Emerg Med. 2014. PMID: 24225332 Clinical Trial.
-
What is the effect of mobile phone text message reminders on medication adherence among adult type 2 diabetes mellitus patients: a systematic review and meta-analysis of randomized controlled trials.BMC Endocr Disord. 2023 Jan 19;23(1):18. doi: 10.1186/s12902-023-01268-8. BMC Endocr Disord. 2023. PMID: 36658577 Free PMC article.
-
Mobile Telephone Text Messaging for Medication Adherence in Chronic Disease: A Meta-analysis.JAMA Intern Med. 2016 Mar;176(3):340-9. doi: 10.1001/jamainternmed.2015.7667. JAMA Intern Med. 2016. PMID: 26831740 Review.
Cited by
-
Feasibility of a Reinforcement Learning-Enabled Digital Health Intervention to Promote Mammograms: Retrospective, Single-Arm, Observational Study.JMIR Form Res. 2022 Nov 28;6(11):e42343. doi: 10.2196/42343. JMIR Form Res. 2022. PMID: 36441579 Free PMC article.
-
Development and Evaluation of a Tailored Mobile Health Intervention to Improve Medication Adherence in Black Patients With Uncontrolled Hypertension and Type 2 Diabetes: Pilot Randomized Feasibility Trial.JMIR Mhealth Uhealth. 2020 Sep 23;8(9):e17135. doi: 10.2196/17135. JMIR Mhealth Uhealth. 2020. PMID: 32965230 Free PMC article. Clinical Trial.
-
Making Inroads in Addressing Population Health in Underserved Communities With Type 2 Diabetes.Diabetes Spectr. 2019 Nov;32(4):303-311. doi: 10.2337/ds19-0010. Diabetes Spectr. 2019. PMID: 31798287 Free PMC article.
-
Disparities in Text Messaging Interventions to Improve Diabetes Management in the United States.Diabetes Spectr. 2021 Jan;34(1):34-41. doi: 10.2337/ds19-0071. Diabetes Spectr. 2021. PMID: 33627992 Free PMC article.
-
The Iterative Convergent Design for Mobile Health Usability Testing: Mixed Methods Approach.JMIR Mhealth Uhealth. 2019 Apr 26;7(4):e11656. doi: 10.2196/11656. JMIR Mhealth Uhealth. 2019. PMID: 31025951 Free PMC article.
References
-
- Hong JS, Kang HC. Relationship between oral antihyperglycemic medication adherence and hospitalization, mortality, and healthcare costs in adult ambulatory care patients with type 2 diabetes in South Korea. Med Care. 2011;49(4):378-384. - PubMed
-
- Krishna S, Boren SA, Balas EA. Healthcare via cell phones: a systematic review. Telemed J E Health. 2009;15(3):231-240. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
