

The serum heart-type fatty acid-binding protein (HFABP) levels can be used to detect the presence of acute kidney injury on admission in patients admitted to the non-surgical intensive care unit
- PMID: 27596162
- PMCID: PMC5011936
- DOI: 10.1186/s12872-016-0340-1
The serum heart-type fatty acid-binding protein (HFABP) levels can be used to detect the presence of acute kidney injury on admission in patients admitted to the non-surgical intensive care unit
Abstract
Background: No cardiac biomarkers for detecting acute kidney injury (AKI) on admission in non-surgical intensive care patients have been reported. The aim of the present study is to elucidate the role of cardiac biomarkers for quickly identifying the presence of AKI on admission.
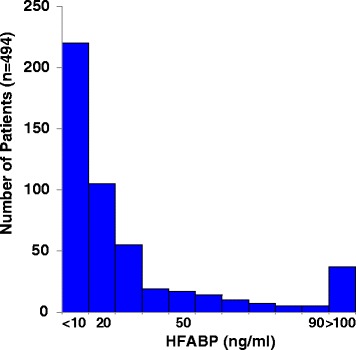
Methods: Data for 1183 patients who underwent the measurement of cardiac biomarkers, including the serum heart-type fatty acid-binding protein (s-HFABP) level, in the emergency department were screened, and 494 non-surgical intensive care patients were enrolled in this study. Based on the RIFLE classification, which was the ratio of the serum creatinine value recorded on admission to the baseline creatinine value, the patients were assigned to a no-AKI (n = 349) or AKI (Class R [n = 83], Class I [n = 36] and Class F [n = 26]) group on admission. We evaluated the diagnostic value of the s-H-FABP level for detecting AKI and Class I/F. The mid-term prognosis, as all-cause death within 180 days, was also evaluated.
Results: The s-H-FABP levels were significantly higher in the Class F (79.2 [29.9 to 200.3] ng/mL) than in the Class I (41.5 [16.7 to 71.6] ng/mL), the Class R (21.1 [10.2 to 47.9] ng/mL), and no-AKI patients (8.8 [5.4 to 17.7] ng/mL). The most predictive values for detecting AKI were Q2 (odds ratio [OR]: 3.743; 95 % confidence interval [CI]: 1.693-8.274), Q3 (OR: 9.427; 95 % CI: 4.124-21.548), and Q4 (OR: 28.000; 95 % CI: 11.245-69.720), while those for Class I/F were Q3 (OR: 5.155; 95 % CI: 1.030-25.790) and Q4 (OR: 22.978; 95 % CI: 4.814-109.668). The s-HFABP level demonstrating an optimal balance between sensitivity and specificity (70.3 and 72.8 %, respectively; area under the curve: 0.774; 95 % CI: 0.728-0.819) was 15.7 ng/mL for AKI and 20.7 ng/mL for Class I/F (71.0 and 83.1 %, respectively; area under the curve: 0.818; 95 % CI: 0.763-0.873). The prognosis was significantly poorer in the high serum HFABP with AKI group than in the other groups.
Conclusions: The s-H-FABP level is an effective biomarker for detecting AKI in non-surgical intensive care patients.
Keywords: Biomarker; Cardiovascular disease; Emergency care; Mortality; Renal dysfunction.
Figures



References
-
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P, Acute Dialysis Quality Initiative workgroup Acute renal failure- definition, outcome measures, animal models, fluid therapy and information technology needs; the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8:R204–12. doi: 10.1186/cc2872. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
