

Differences in GlycA and lipoprotein particle parameters may help distinguish acute kawasaki disease from other febrile illnesses in children
- PMID: 27596163
- PMCID: PMC5011873
- DOI: 10.1186/s12887-016-0688-5
Differences in GlycA and lipoprotein particle parameters may help distinguish acute kawasaki disease from other febrile illnesses in children
Abstract
Background: Glycosylation patterns of serum proteins, such as α1-acid glycoprotein, are modified during an acute phase reaction. The response of acute Kawasaki disease (KD) patients to IVIG treatment has been linked to sialic acid levels on native IgG, suggesting that protein glycosylation patterns vary during the immune response in acute KD. Additionally, the distribution and function of lipoprotein particles are altered during inflammation. Therefore, the aim of this study was to explore the potential for GlycA, a marker of protein glycosylation, and the lipoprotein particle profile to distinguish pediatric patients with acute KD from those with other febrile illnesses.
Methods: Nuclear magnetic resonance was used to quantify GlycA and lipoprotein particle classes and subclasses in pediatric subjects with acute KD (n = 75), post-treatment subacute (n = 36) and convalescent (n = 63) KD, as well as febrile controls (n = 48), and age-similar healthy controls (n = 48).
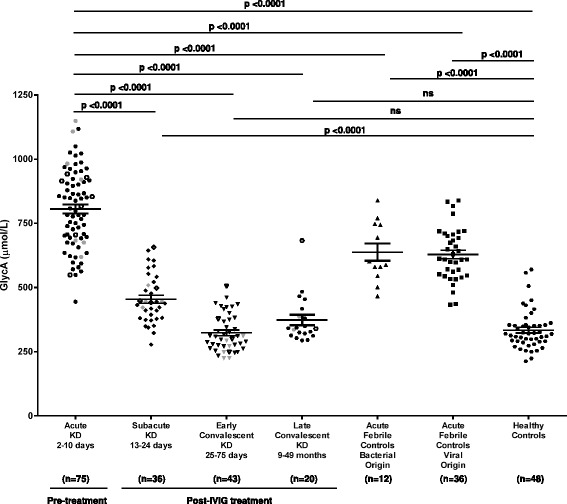
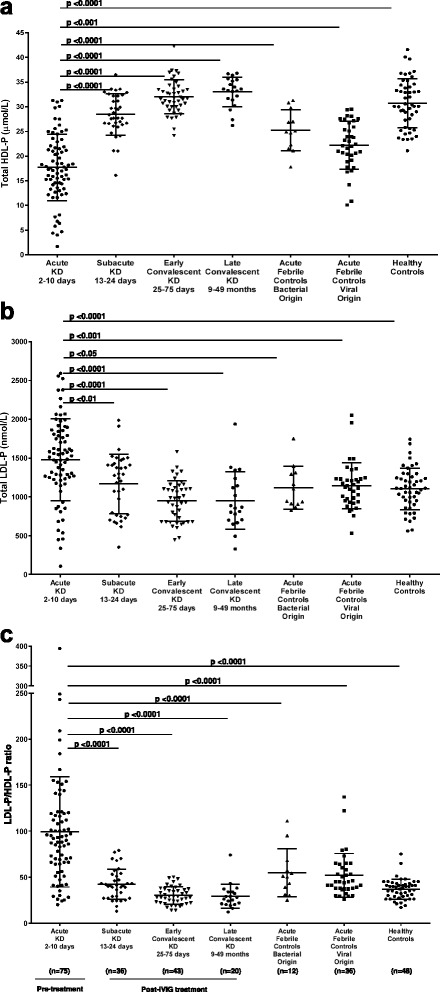
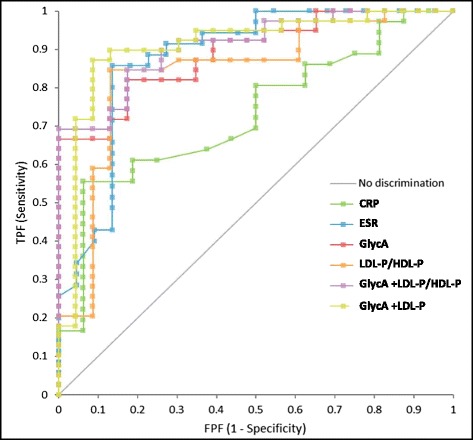
Results: GlycA was elevated in acute KD subjects compared to febrile controls with bacterial or viral infections, IVIG-treated subacute and convalescent KD subjects, and healthy children (P <0.0001). Acute KD subjects had increased total and small low density lipoprotein particle numbers (LDL-P) (P <0.0001) and decreased total high density lipoprotein particle number (HDL-P) (P <0.0001) compared to febrile controls. Consequently, the ratio of LDL-P to HDL-P was higher in acute KD subjects than all groups tested (P <0.0001). While GlycA, CRP, erythrocyte sedimentation rate, LDL-P and LDL-P/HDL-P ratio were able to distinguish patients with KD from those with other febrile illnesses (AUC = 0.789-0.884), the combinations of GlycA and LDL-P (AUC = 0.909) or GlycA and the LDL-P/HDL-P ratio (AUC = 0.910) were best at discerning KD in patients 6-10 days after illness onset.
Conclusions: High levels of GlycA confirm enhanced protein glycosylation as part of the acute phase response in KD patients. When combined with common laboratory tests and clinical characteristics, GlycA and NMR-measured lipoprotein particle parameters may be useful for distinguishing acute KD from bacterial or viral illnesses in pediatric patients.
Keywords: Biomarkers; GlycA; Kawasaki disease; Lipoprotein particle number.
Figures
Similar articles
-
Primary aldosteronism is associated with decreased low-density and high-density lipoprotein particle concentrations and increased GlycA, a pro-inflammatory glycoprotein biomarker.Clin Endocrinol (Oxf). 2019 Jan;90(1):79-87. doi: 10.1111/cen.13891. Epub 2018 Nov 20. Clin Endocrinol (Oxf). 2019. PMID: 30372543
-
Lipoprotein particle concentrations in children and adults following Kawasaki disease.J Pediatr. 2014 Oct;165(4):727-31. doi: 10.1016/j.jpeds.2014.06.017. Epub 2014 Jul 16. J Pediatr. 2014. PMID: 25039043 Free PMC article.
-
Pro-brain natriuretic peptide (ProBNP) levels in North Indian children with Kawasaki disease.Rheumatol Int. 2016 Apr;36(4):551-9. doi: 10.1007/s00296-016-3430-6. Epub 2016 Feb 5. Rheumatol Int. 2016. PMID: 26849890
-
Fifteen-minute consultation: Kawasaki disease: how to distinguish from other febrile illnesses: tricks and tips.Arch Dis Child Educ Pract Ed. 2020 Jun;105(3):152-156. doi: 10.1136/archdischild-2019-316834. Epub 2020 Jan 3. Arch Dis Child Educ Pract Ed. 2020. PMID: 31900257 Review.
-
Diagnostic significance of circulating miRNAs in Kawasaki disease in China: Current evidence based on a meta-analysis.Medicine (Baltimore). 2021 Feb 12;100(6):e24174. doi: 10.1097/MD.0000000000024174. Medicine (Baltimore). 2021. PMID: 33578520 Free PMC article.
Cited by
-
Increased glycoprotein acetylation is associated with high cardiac event rates: Analysis using coronary computed tomography angiography.Anatol J Cardiol. 2018 Sep;20(3):152-158. doi: 10.14744/AnatolJCardiol.2018.01058. Anatol J Cardiol. 2018. PMID: 30152796 Free PMC article.
-
Glycoprotein Profile Measured by a 1H-Nuclear Magnetic Resonance Based on Approach in Patients with Diabetes: A New Robust Method to Assess Inflammation.Life (Basel). 2021 Dec 16;11(12):1407. doi: 10.3390/life11121407. Life (Basel). 2021. PMID: 34947938 Free PMC article.
-
GlycA, a novel biomarker of systemic inflammation and cardiovascular disease risk.J Transl Med. 2017 Oct 27;15(1):219. doi: 10.1186/s12967-017-1321-6. J Transl Med. 2017. PMID: 29078787 Free PMC article. Review.
-
Title: Human Serum/Plasma Glycoprotein Analysis by 1H-NMR, an Emerging Method of Inflammatory Assessment.J Clin Med. 2020 Jan 27;9(2):354. doi: 10.3390/jcm9020354. J Clin Med. 2020. PMID: 32012794 Free PMC article. Review.
-
Evidence of a genetically driven metabolomic signature in actively inflamed Crohn's disease.Sci Rep. 2022 Aug 18;12(1):14101. doi: 10.1038/s41598-022-18178-9. Sci Rep. 2022. PMID: 35982195 Free PMC article.
References
-
- Kawasaki T, Kosaki F, Okawa S, Shigematsu I, Yanagawa H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics. 1974;54(3):271–276. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
