

Liver fibrosis in treatment-naïve HIV-infected and HIV/HBV co-infected patients: Zambia and Switzerland compared
- PMID: 27596685
- PMCID: PMC5363287
- DOI: 10.1016/j.ijid.2016.08.028
Liver fibrosis in treatment-naïve HIV-infected and HIV/HBV co-infected patients: Zambia and Switzerland compared
Abstract
Objective: To examine the association between hepatitis B virus (HBV) infection and liver fibrosis in HIV-infected patients in Zambia and Switzerland.
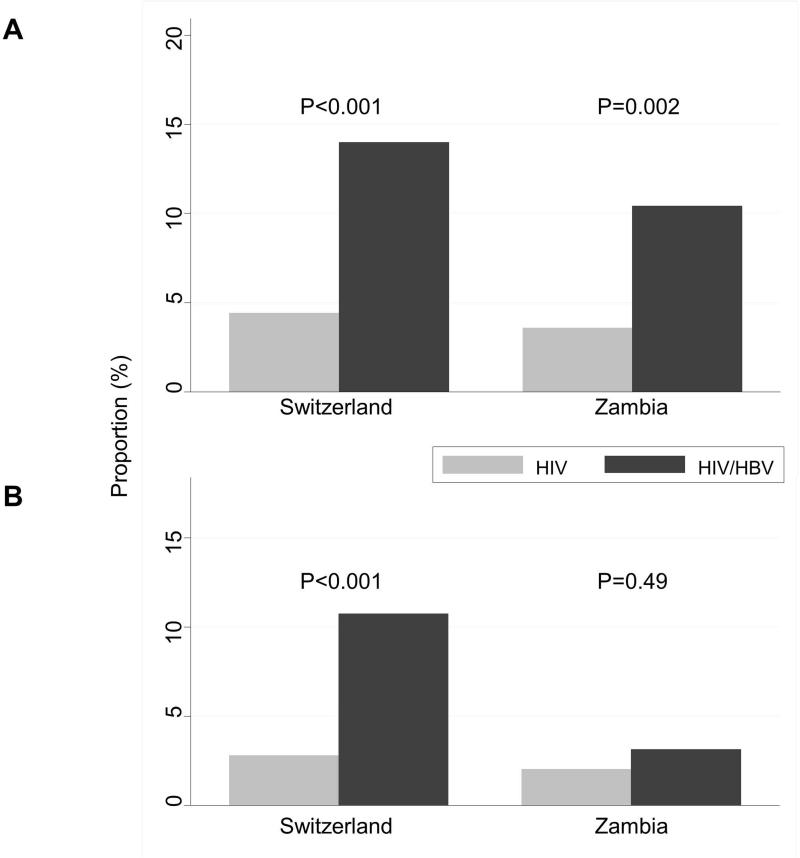
Methods: HIV-infected adults starting antiretroviral therapy in two clinics in Zambia and Switzerland were included. Liver fibrosis was evaluated using the aspartate aminotransferase-to-platelet-ratio index (APRI), with a ratio >1.5 defining significant fibrosis and a ratio >2.0 indicating cirrhosis. The association between hepatitis B surface antigen (HBsAg) positivity, HBV replication, and liver fibrosis was examined using logistic regression.
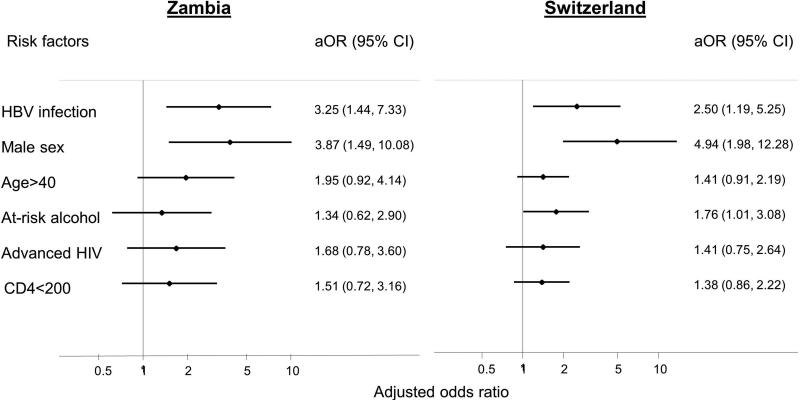
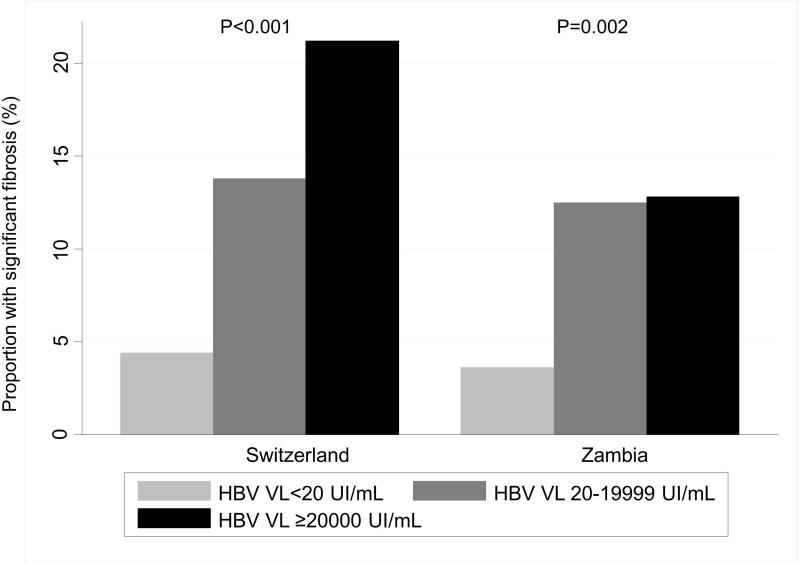
Results: In Zambia, 96 (13.0%) of 739 patients were HBsAg-positive compared to 93 (4.5%) of 2058 in Switzerland. HBsAg-positive patients were more likely to have significant liver fibrosis than HBsAg-negative ones: the adjusted odds ratio (aOR) was 3.25 (95% confidence interval (CI) 1.44-7.33) in Zambia and 2.50 (95% CI 1.19-5.25) in Switzerland. Patients with a high HBV viral load (≥20000 IU/ml) were more likely to have significant liver fibrosis compared to HBsAg-negative patients or patients with an undetectable viral load: aOR 3.85 (95% CI 1.29-11.44) in Zambia and 4.20 (95% CI 1.64-10.76) in Switzerland. In both settings, male sex was a strong risk factor for significant liver fibrosis.
Conclusions: Despite the differences in HBV natural history between Sub-Saharan Africa and Europe, the degree of liver fibrosis and the association with important risk factors were similar.
Keywords: HIV; Hepatitis B infection; Liver fibrosis; Switzerland; Zambia.
Copyright © 2016 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Weber R, Sabin CA, Friis-Moller N, Reiss P, El-Sadr WM, Kirk O, et al. Liver-related deaths in persons infected with the human immunodeficiency virus: the D:A:D study. Arch Intern Med. 2006;166(15):1632–41. - PubMed
-
- Perz JF, Armstrong GL, Farrington LA, Hutin YJ, Bell BP. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol. 2006;45(4):529–38. - PubMed
-
- Thio CL, Seaberg EC, Skolasky R, Jr., Phair J, Visscher B, Munoz A, et al. HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet. 2002;360(9349):1921–6. - PubMed
-
- Fattovich G, Bortolotti F, Donato F. Natural history of chronic hepatitis B: special emphasis on disease progression and prognostic factors. J Hepatol. 2008;48(2):335–52. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
