

Pre-operative echocardiography among patients with coronary artery disease in the United States Veterans Affairs healthcare system: A retrospective cohort study
- PMID: 27596717
- PMCID: PMC5011899
- DOI: 10.1186/s12872-016-0357-5
Pre-operative echocardiography among patients with coronary artery disease in the United States Veterans Affairs healthcare system: A retrospective cohort study
Abstract
Background: Echocardiography is not recommended for routine pre-surgical evaluation but may have value for patients at high risk of major adverse cardiovascular events (MACE). The objective of this study was to evaluate whether pre-operative echocardiography is associated with lower risk of post-operative MACE among patients with coronary artery disease.
Methods: Using administrative and registry data, we examined associations of echocardiography within 3 months prior to surgery with postoperative MACE (myocardial infarction, revascularization, or death within 30 days) among patients with coronary artery disease undergoing elective, non-cardiac surgeries in the United States Veterans Affairs healthcare system in 2000-2012.
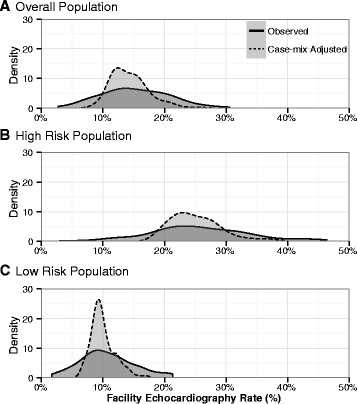
Results: Echocardiography preceded 4,378 (16.4 %) of 26,641 surgeries. MACE occurred within 30 days following 944 (3.5 %) surgeries. A 10 % higher case-mix adjusted rate of pre-operative echocardiography assessed at the hospital level was associated with a hospital-level risk of MACE that was 1.0 % (95 % confidence interval [CI] 0.1 %, 2.0 %) higher overall and 1.7 % (95 % CI 0.2 %, 3.2 %) higher among patients with recent myocardial infarction, valvular heart disease, or heart failure. At the patient level, pre-operative echocardiography was associated with an odds ratio for MACE of 1.9 (95 % CI 1.7, 2.2) overall and 1.8 (95 % CI 1.5, 2.2) among patients with recent myocardial infarction, valvular heart disease, or heart failure adjusting for MACE risk factors.
Conclusions: Pre-operative echocardiography was not associated with lower risk of post-operative MACE, even in a high risk population. Future guidelines should encourage pre-operative echocardiography only in specific patients with cardiovascular disease among whom findings can be translated into effective changes in care.
Keywords: Echocardiography; Major adverse cardiac events; Surgery.
Figures


References
-
- Wijeysundera DN, Beattie WS, Karkouti K, Neuman MD, Austin PC, Laupacis A. Association of echocardiography before major elective non-cardiac surgery with postoperative survival and length of hospital stay: population based cohort study. BMJ. 2011;342:d3695. doi: 10.1136/bmj.d3695. - DOI - PMC - PubMed
-
- American College of Cardiology Foundation Appropriate Use Criteria Task F, American Society of E, American Heart A, American Society of Nuclear C, Heart Failure Society of A, Heart Rhythm S, Society for Cardiovascular A, Interventions, Society of Critical Care M, Society of Cardiovascular Computed T et al. ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 Appropriate Use Criteria for Echocardiography. A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Society of Echocardiography, American Heart Association, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Critical Care Medicine, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance Endorsed by the American College of Chest Physicians. J Am Coll Cardiol. 2011;57(9):1126–1166. doi: 10.1016/j.jacc.2010.11.002. - DOI - PubMed
-
- Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, Davila-Roman VG, Gerhard-Herman MD, Holly TA, Kane GC, et al. ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e77–137. doi: 10.1016/j.jacc.2014.07.944. - DOI - PubMed
-
- American Society of Echocardiography Five Things Physicians and Patients Should Question. 2013. http://www.choosingwisely.org/doctor-patient-lists/american-society-of-e.... Accessed 24 Mar 2015.
-
- Task Force for Preoperative Cardiac Risk A, Perioperative Cardiac Management in Non-cardiac S, European Society of C. Poldermans D, Bax JJ, Boersma E, De Hert S, Eeckhout E, Fowkes G, Gorenek B, et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. Eur Heart J. 2009;30(22):2769–2812. doi: 10.1093/eurheartj/ehp337. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
