

Identification of Site-specific Recurrence Following Primary Radiation Therapy for Prostate Cancer Using C-11 Choline Positron Emission Tomography/Computed Tomography: A Nomogram for Predicting Extrapelvic Disease
- PMID: 27597240
- PMCID: PMC5729924
- DOI: 10.1016/j.eururo.2016.08.055
Identification of Site-specific Recurrence Following Primary Radiation Therapy for Prostate Cancer Using C-11 Choline Positron Emission Tomography/Computed Tomography: A Nomogram for Predicting Extrapelvic Disease
Abstract
Background: Management of recurrent prostate cancer (CaP) after radiotherapy (RT) is dependent on accurate localization of the site of recurrent disease.
Objective: To describe the anatomic patterns and clinical features associated with CaP recurrence following RT identified on advanced imaging.
Design, setting, and participants: Retrospective review of 184 patients with a rising prostate-specific antigen (PSA) after RT for CaP.
Intervention: C-11 choline positron emission tomography/computed tomography (CholPET).
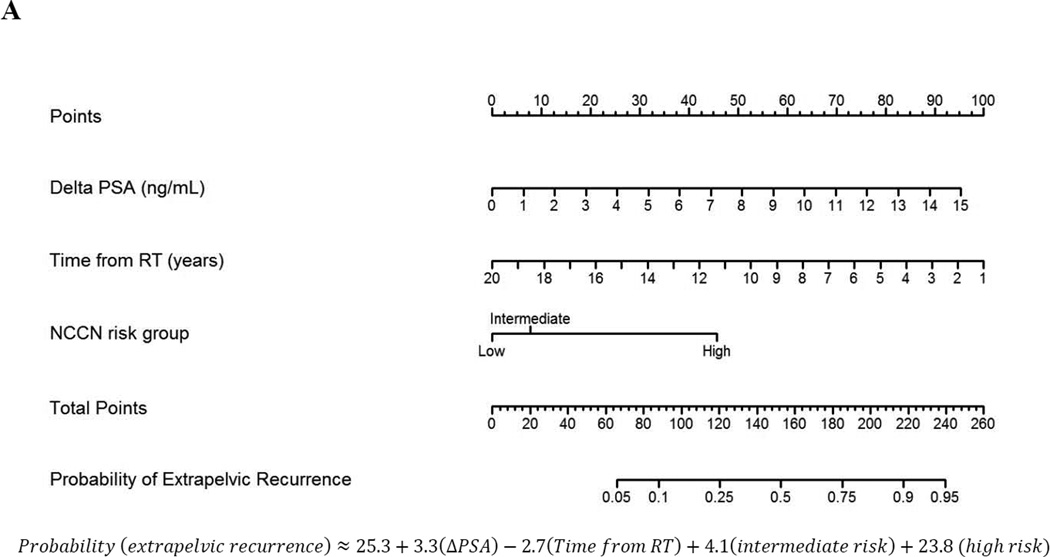
Outcome measurements and statistical analysis: Recurrence patterns were classified as pelvic soft tissue only (as a surrogate for potentially salvageable disease) versus any extrapelvic disease, and clinical features were compared between patterns. Multivariable logistic regression was used to generate a predictive nomogram for extrapelvic recurrence. Discrimination was assessed with a c-index.
Results and limitations: Recurrence site was identified in 161 (87%) patients, with 95 (59%) sites histologically confirmed. Factors associated with the detection of recurrence included the difference between PSA nadir and PSA at CholPET (odds ratio: 1.30, p<0.01) and National Comprehensive Cancer Network high-risk classification (odds ratio: 10.83, p=0.03). One hundred (54.3%) patients recurred in the pelvic soft tissue only, while 61 (33%) had extrapelvic recurrence. Of 21 patients who underwent CholPET prior to meeting the Phoenix criteria of biochemical failure, 15 (71%) had recurrence identified on CholPET with 11 localized to the pelvis. On multivariable analysis, the difference between PSA nadir and PSA at CholPET, time from RT, and National Comprehensive Cancer Network risk group were predictive of recurrence outside of the pelvis, and a nomogram was generated with a c-index of 0.79.
Conclusions: CholPET identified the site of recurrence in 87% of patients with a rising PSA after RT; most commonly within the pelvis in potentially salvageable locations. A predictive nomogram was generated, and pending external validation, this may aid in assessing the risk of disease beyond the pelvis. These findings underscore the importance of advanced imaging when considering management strategies for patients with a rising PSA following primary RT.
Patient summary: We identified anatomic patterns of recurrence in patients with a rising prostate-specific antigen after radiotherapy using C-11 choline positron emission tomography/computed tomography. Most recurrences were localized to the pelvis and we were able to generate a tool to aid in disease localization prior to evaluation with advanced imaging.
Keywords: Nomogram; PET/CT; Prostate Cancer; Radiation Therapy; Recurrence.
Copyright © 2016 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Choline Positron Emission Tomography/Computed Tomography for Selection of Patients for Salvage Strategies After Primary Local Treatment of Prostate Cancer and Rising Prostate-specific Antigen: Ready for Prime Time?Eur Urol. 2017 Mar;71(3):349-350. doi: 10.1016/j.eururo.2016.10.051. Epub 2016 Nov 11. Eur Urol. 2017. PMID: 27842722 No abstract available.
-
Reply from Authors re: Alberto Bossi, Nicolas Mottet, Pierre Blanchard. Choline Positron Emission Tomography/Computed Tomography for Selection of Patients for Salvage Strategies After Primary Local Treatment of Prostate Cancer and Rising Prostate-specific Antigen: Ready for Prime Time? Eur Urol 2017;71:349-50: C-11 Choline PET/CT and Guideline-directed Care.Eur Urol. 2017 Mar;71(3):351-352. doi: 10.1016/j.eururo.2016.11.022. Epub 2016 Nov 30. Eur Urol. 2017. PMID: 27914899 No abstract available.
References
-
- Roach M, 3rd, Hanks G, Thames H, Jr, et al. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys. 2006;65:965–974. - PubMed
-
- Denham JW, Steigler A, Wilcox C, et al. Why are pretreatment prostate-specific antigen levels and biochemical recurrence poor predictors of prostate cancer survival? Cancer. 2009;115:4477–4487. - PubMed
-
- Morris LM, Izard MA, Wan WY. Does prostate-specific antigen nadir predict longer-term outcomes of prostate cancer after neoadjuvant and adjuvant androgen deprivation therapy in conjunction with brachytherapy? Brachytherapy. 2015;14:322–328. - PubMed
-
- Uchio E, Aslan M, Ko J, Wells CK, Radhakrishnan K, Concato J. Velocity and doubling time of prostate-specific antigen: Mathematics can matter. J Investig Med. 2016;64:400–404. - PubMed
-
- Chade DC, Eastham J, Graefen M, et al. Cancer control and functional outcomes of salvage radical prostatectomy for radiation-recurrent prostate cancer: A systematic review of the literature. Eur Urol. 2012;61:961–971. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
