

The Reality of Myoelectric Prostheses: Understanding What Makes These Devices Difficult for Some Users to Control
- PMID: 27597823
- PMCID: PMC4992705
- DOI: 10.3389/fnbot.2016.00007
The Reality of Myoelectric Prostheses: Understanding What Makes These Devices Difficult for Some Users to Control
Erratum in
-
Corrigendum: The Reality of Myoelectric Prostheses: Understanding What Makes These Devices Difficult for Some Users to Control.Front Neurorobot. 2018 Apr 3;12:15. doi: 10.3389/fnbot.2018.00015. eCollection 2018. Front Neurorobot. 2018. PMID: 29643774 Free PMC article.
Abstract
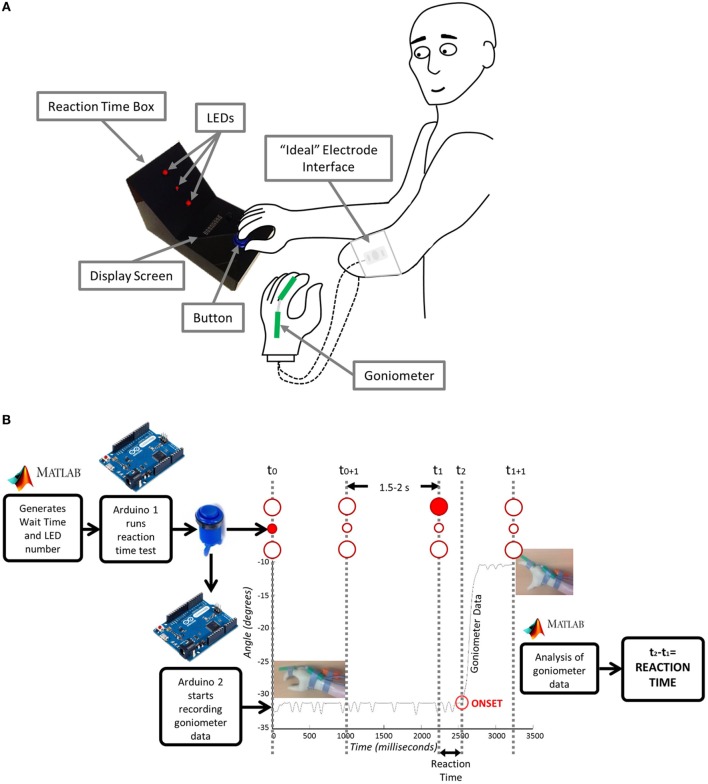
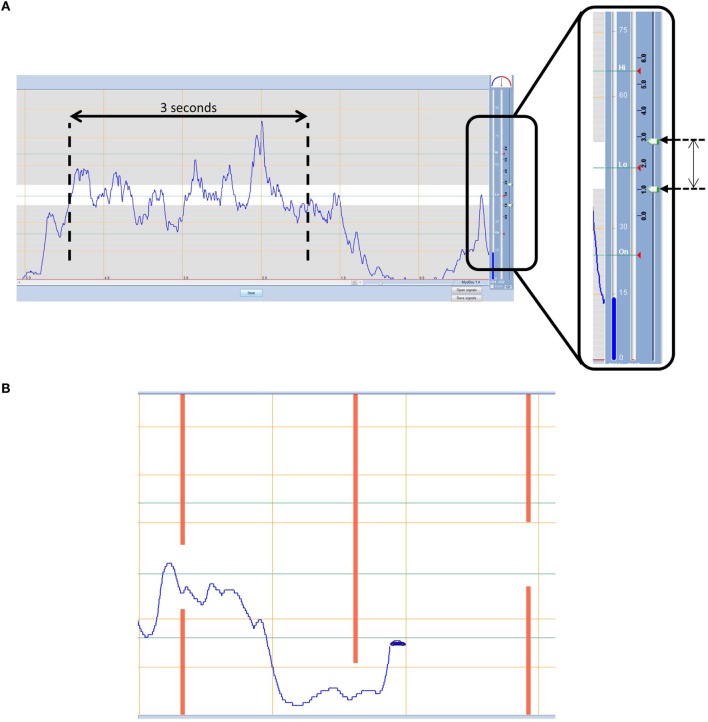
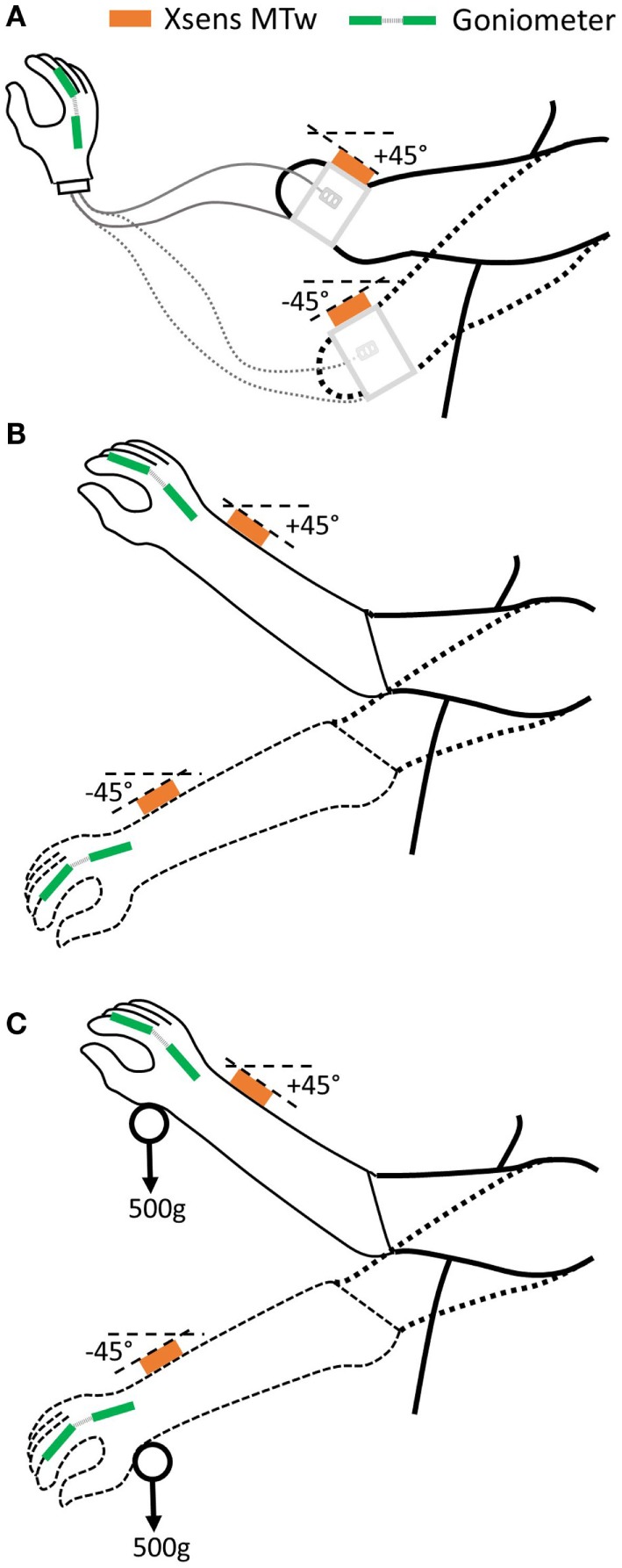
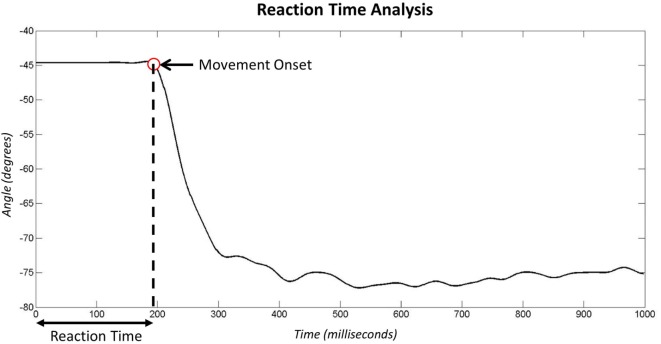
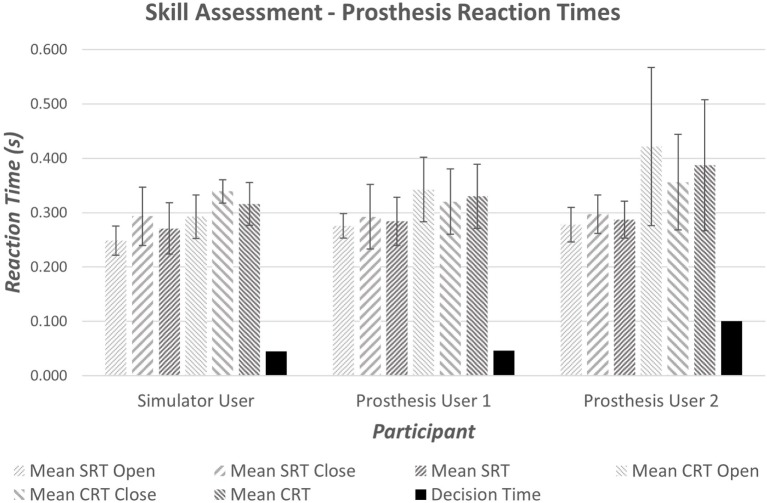
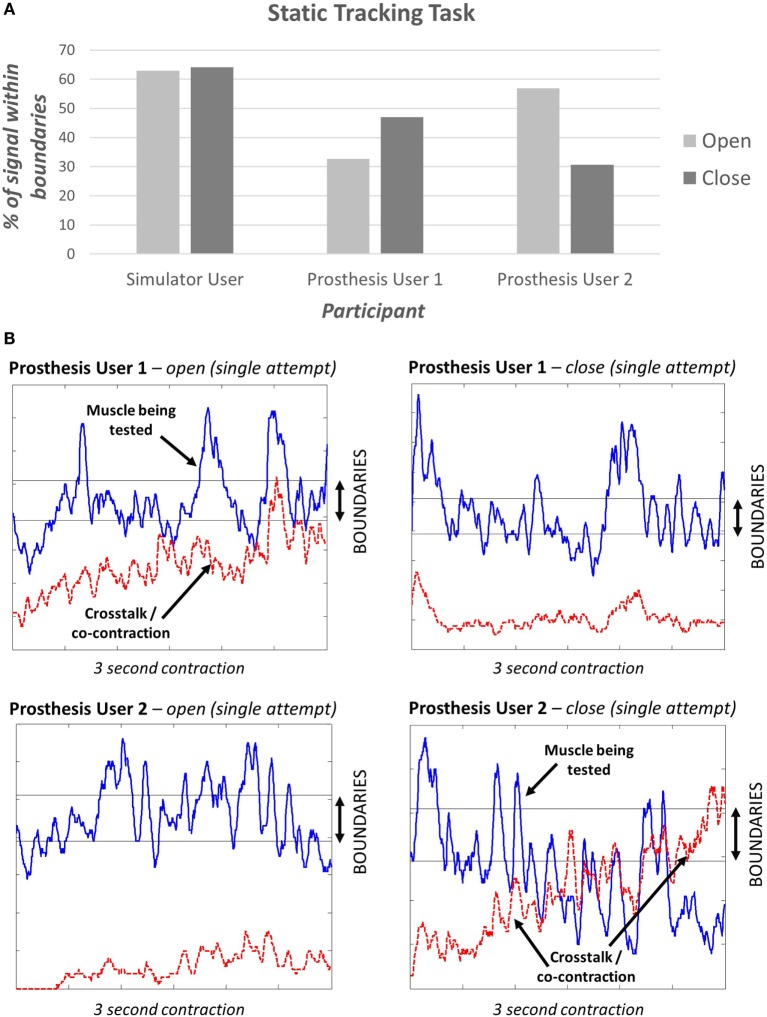
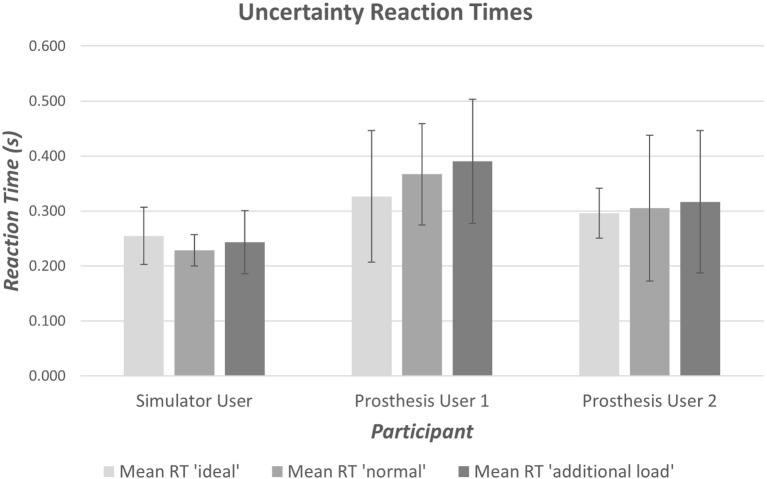
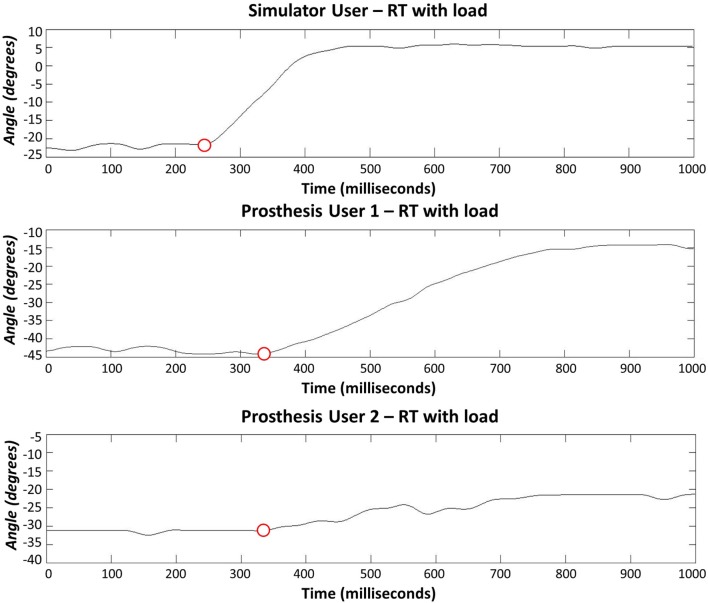
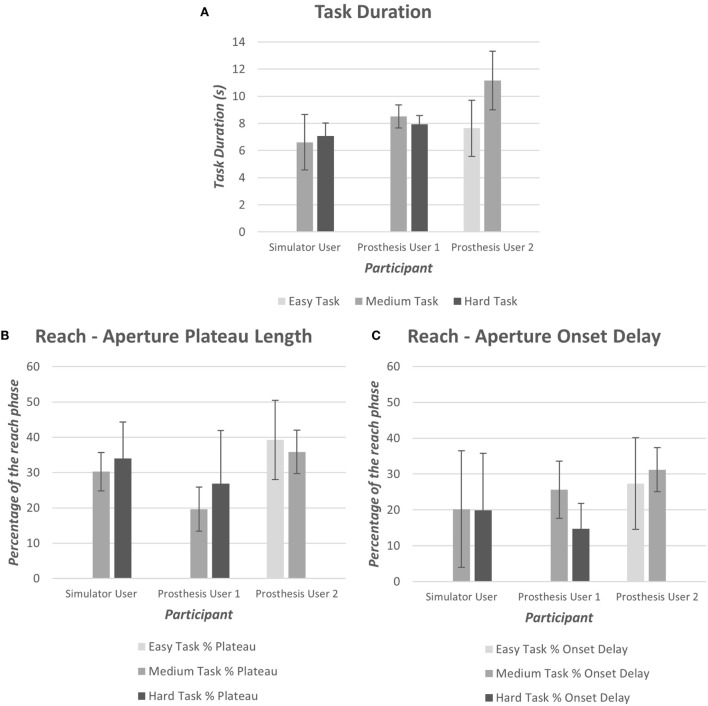
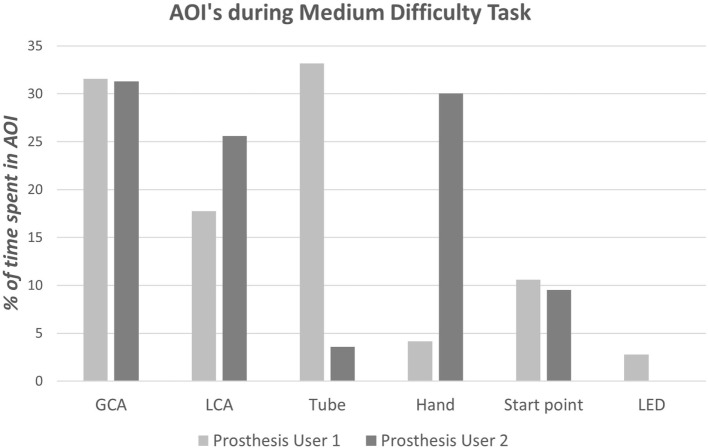
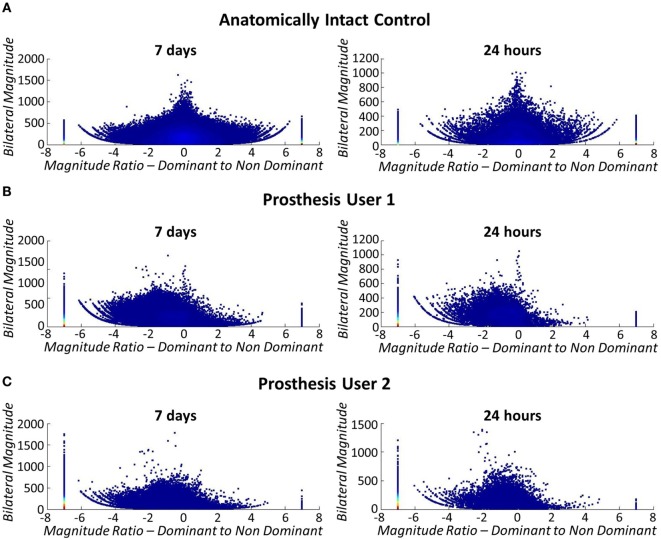
Users of myoelectric prostheses can often find them difficult to control. This can lead to passive-use of the device or total rejection, which can have detrimental effects on the contralateral limb due to overuse. Current clinically available prostheses are "open loop" systems, and although considerable effort has been focused on developing biofeedback to "close the loop," there is evidence from laboratory-based studies that other factors, notably improving predictability of response, may be as, if not more, important. Interestingly, despite a large volume of research aimed at improving myoelectric prostheses, it is not currently known which aspect of clinically available systems has the greatest impact on overall functionality and everyday usage. A protocol has, therefore, been designed to assess electromyographic (EMG) skill of the user and predictability of the prosthesis response as significant parts of the control chain, and to relate these to functionality and everyday usage. Here, we present the protocol and results from early pilot work. A set of experiments has been developed. First, to characterize user skill in generating the required level of EMG signal, as well as the speed with which users are able to make the decision to activate the appropriate muscles. Second, to measure unpredictability introduced at the skin-electrode interface, in order to understand the effects of the socket-mounted electrode fit under different loads on the variability of time taken for the prosthetic hand to respond. To evaluate prosthesis user functionality, four different outcome measures are assessed. Using a simple upper limb functional task prosthesis users are assessed for (1) success of task completion, (2) task duration, (3) quality of movement, and (4) gaze behavior. To evaluate everyday usage away from the clinic, the symmetricity of their real-world arm use is assessed using activity monitoring. These methods will later be used to assess a prosthesis user cohort to establish the relative contribution of each control factor to the individual measures of functionality and everyday usage (using multiple regression models). The results will support future researchers, designers, and clinicians in concentrating their efforts on the area that will have the greatest impact on improving prosthesis use.
Keywords: activity monitoring; control; functionality assessment; myoelectric; prosthesis; upper limb.
Figures



References
-
- Actigraph Corp. (2015). ActiGraph White Paper: What Is a Count? Pensacola, FL.
LinkOut - more resources
Full Text Sources
Other Literature Sources