

The pretreatment Controlling Nutritional Status (CONUT) score is an independent prognostic factor in patients with resectable thoracic esophageal squamous cell carcinoma: results from a retrospective study
- PMID: 27599460
- PMCID: PMC5013653
- DOI: 10.1186/s12885-016-2696-0
The pretreatment Controlling Nutritional Status (CONUT) score is an independent prognostic factor in patients with resectable thoracic esophageal squamous cell carcinoma: results from a retrospective study
Abstract
Background: The purpose of this study was to investigate the impact of the Controlling Nutritional Status (CONUT) score on survival compared with the platelet to lymphocyte ratio (PLR), the neutrophil to lymphocyte ratio (NLR), and the Glasgow Prognostic Score (GPS) in patients with resectable thoracic esophageal squamous cell carcinoma (ESCC).
Methods: One hundred eighty-five consecutive patients who underwent subtotal esophagectomy with curative intent for resectable thoracic ESCC were retrospectively reviewed. Time-dependent receiver operating characteristic curve analyses for 3-year overall survival (OS) as the endpoint were performed, and the maximal Youden indices were calculated to assess discrimination ability and to determine the appropriate cut-off values of CONUT, PLR, and NLR. The patients were then classified into high and low groups based on these cut-off values. Correlations between CONUT and other clinicopathological characteristics were analyzed. Prognostic factors predicting overall survival (OS) and relapse-free survival (RFS) were analyzed using Cox proportional hazards models.
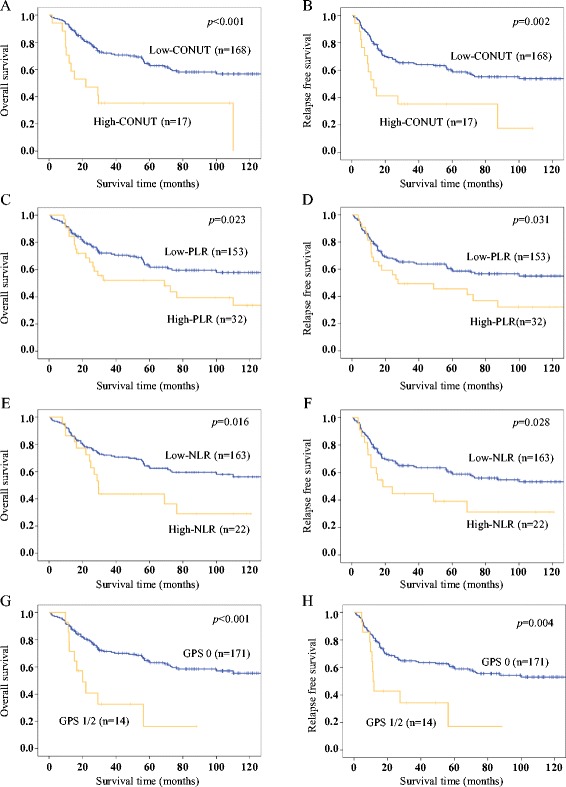
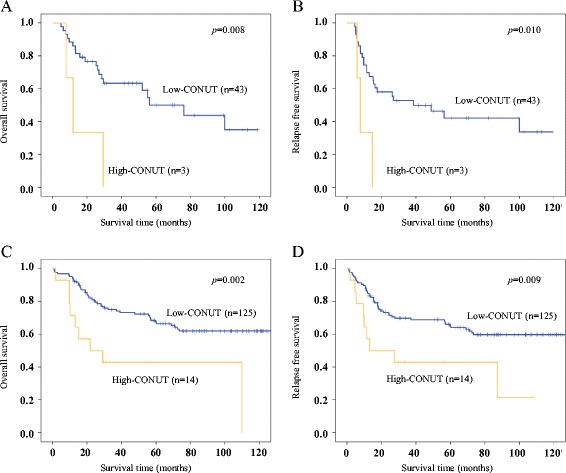
Results: The areas under the curve predicting 3-year OS were 0.603 for CONUT, 0.561 for PLR, 0.564 for NLR, and 0.563 for GPS. The optimal cut-off values were two for the CONUT score, 193 for PLR, and 3.612 for NLR. The high-CONUT group was significantly associated with lower BMI, high-PLR, high-NLR, and GPS1/2 groups. On univariate analysis, high-CONUT, high-PLR, high-NLR, and GPS 1/2 groups were significantly associated with poorer OS and RFS. Of these factors, multivariate analysis revealed that only the CONUT score was an independent prognostic factor for OS (HR 2.303, 95 % CI 1.191-4.455; p = 0.013) and RFS (HR 2.163, 95 % CI 1.139-4.109; p = 0.018).
Conclusions: The CONUT score was an independent predictor of OS and RFS before treatment and was superior to PLR, NLR, and GPS in terms of predictive ability for prognosis in patients with resectable thoracic ESCC.
Keywords: Controlling nutritional status; Esophageal cancer; Esophagectomy; Nutrition; Prognostic factor.
Figures
Similar articles
-
Prognostic significance of preoperative lymphocyte-monocyte ratio in patients with resectable esophageal squamous cell carcinoma.Asian Pac J Cancer Prev. 2015;16(6):2245-50. doi: 10.7314/apjcp.2015.16.6.2245. Asian Pac J Cancer Prev. 2015. PMID: 25824745
-
Prognostic value of the neutrophil-to-lymphocyte ratio for overall and disease-free survival in patients with surgically treated esophageal squamous cell carcinoma.Tumour Biol. 2016 Jun;37(6):7149-54. doi: 10.1007/s13277-015-4596-3. Epub 2015 Dec 12. Tumour Biol. 2016. PMID: 26662960
-
Prognostic value of preoperative platelet-lymphocyte and neutrophil-lymphocyte ratio in patients undergoing surgery for esophageal squamous cell cancer.Dis Esophagus. 2016 Jan;29(1):79-85. doi: 10.1111/dote.12296. Epub 2014 Nov 19. Dis Esophagus. 2016. PMID: 25410116
-
Prognostic Potential of the Preoperative Controlling Nutritional Status (CONUT) Score in Predicting Survival of Patients with Cancer: A Systematic Review.Adv Nutr. 2021 Feb 1;12(1):234-250. doi: 10.1093/advances/nmaa102. Adv Nutr. 2021. PMID: 32910812 Free PMC article.
-
Prognostic roles of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in ovarian cancer: a meta-analysis of retrospective studies.Arch Gynecol Obstet. 2018 Apr;297(4):849-857. doi: 10.1007/s00404-018-4678-8. Epub 2018 Jan 24. Arch Gynecol Obstet. 2018. PMID: 29368160 Review.
Cited by
-
The Clinical Influence of the CONUT Score on Survival of Patients With Gastric Cancer Receiving Curative Treatment.In Vivo. 2022 Mar-Apr;36(2):942-948. doi: 10.21873/invivo.12784. In Vivo. 2022. PMID: 35241553 Free PMC article.
-
Prognostic Value of Combined Tumor Marker and Controlling Nutritional Status (CONUT) Score in Colorectal Cancer Patients.Yonago Acta Med. 2019 Mar 28;62(1):124-130. doi: 10.33160/yam.2019.03.017. eCollection 2019 Mar. Yonago Acta Med. 2019. PMID: 30962754 Free PMC article.
-
Naples Prognostic Score Predicts Tumor Regression Grade in Resectable Gastric Cancer Treated with Preoperative Chemotherapy.Cancers (Basel). 2021 Sep 17;13(18):4676. doi: 10.3390/cancers13184676. Cancers (Basel). 2021. PMID: 34572903 Free PMC article.
-
Refining Nutritional Assessment Methods for Older Adults: A Pilot Study on Sicilian Long-Living Individuals.Nutrients. 2025 May 30;17(11):1873. doi: 10.3390/nu17111873. Nutrients. 2025. PMID: 40507142 Free PMC article.
-
Prognostic value of an inflammation-based nutritional score for patients with initially unresectable pancreatic adenocarcinoma undergoing conversion surgery following chemo-/radiotherapy.Surg Today. 2021 Oct;51(10):1682-1693. doi: 10.1007/s00595-021-02279-5. Epub 2021 Apr 7. Surg Today. 2021. PMID: 33829334
References
-
- Ando N, Kato H, Igaki H, et al. A randomized trial comparing postoperative adjuvant chemotherapy with cisplatin and 5-fluorouracil versus preoperative chemotherapy for localized advanced squamous cell carcinoma of the thoracic esophagus (JCOG9907) Ann Surg Oncol. 2012;19(1):68–74. doi: 10.1245/s10434-011-2049-9. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
