

Prospective risk of stillbirth and neonatal complications in twin pregnancies: systematic review and meta-analysis
- PMID: 27599496
- PMCID: PMC5013231
- DOI: 10.1136/bmj.i4353
Prospective risk of stillbirth and neonatal complications in twin pregnancies: systematic review and meta-analysis
Abstract
Objective: To determine the risks of stillbirth and neonatal complications by gestational age in uncomplicated monochorionic and dichorionic twin pregnancies.
Design: Systematic review and meta-analysis.
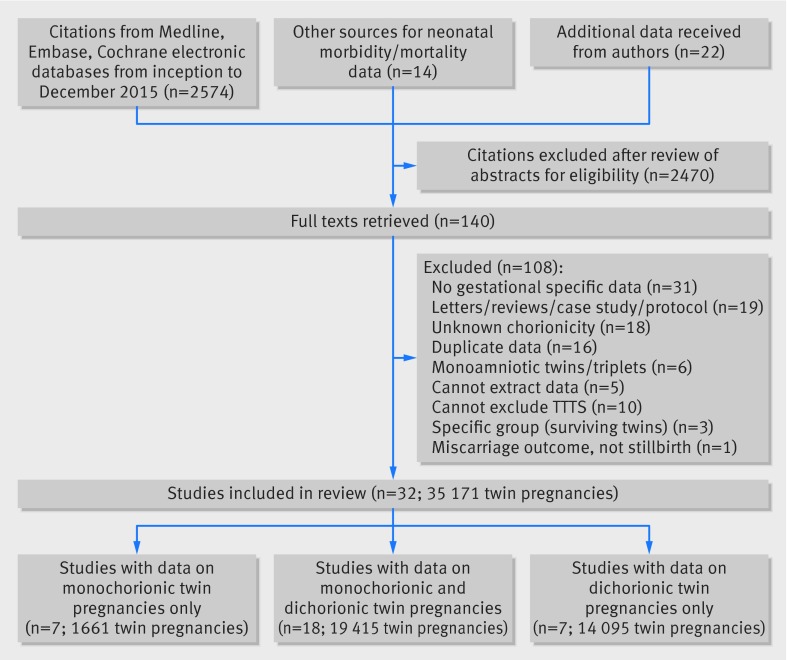
Data sources: Medline, Embase, and Cochrane databases (until December 2015).
Review methods: Databases were searched without language restrictions for studies of women with uncomplicated twin pregnancies that reported rates of stillbirth and neonatal outcomes at various gestational ages. Pregnancies with unclear chorionicity, monoamnionicity, and twin to twin transfusion syndrome were excluded. Meta-analyses of observational studies and cohorts nested within randomised studies were undertaken. Prospective risk of stillbirth was computed for each study at a given week of gestation and compared with the risk of neonatal death among deliveries in the same week. Gestational age specific differences in risk were estimated for stillbirths and neonatal deaths in monochorionic and dichorionic twin pregnancies after 34 weeks' gestation.
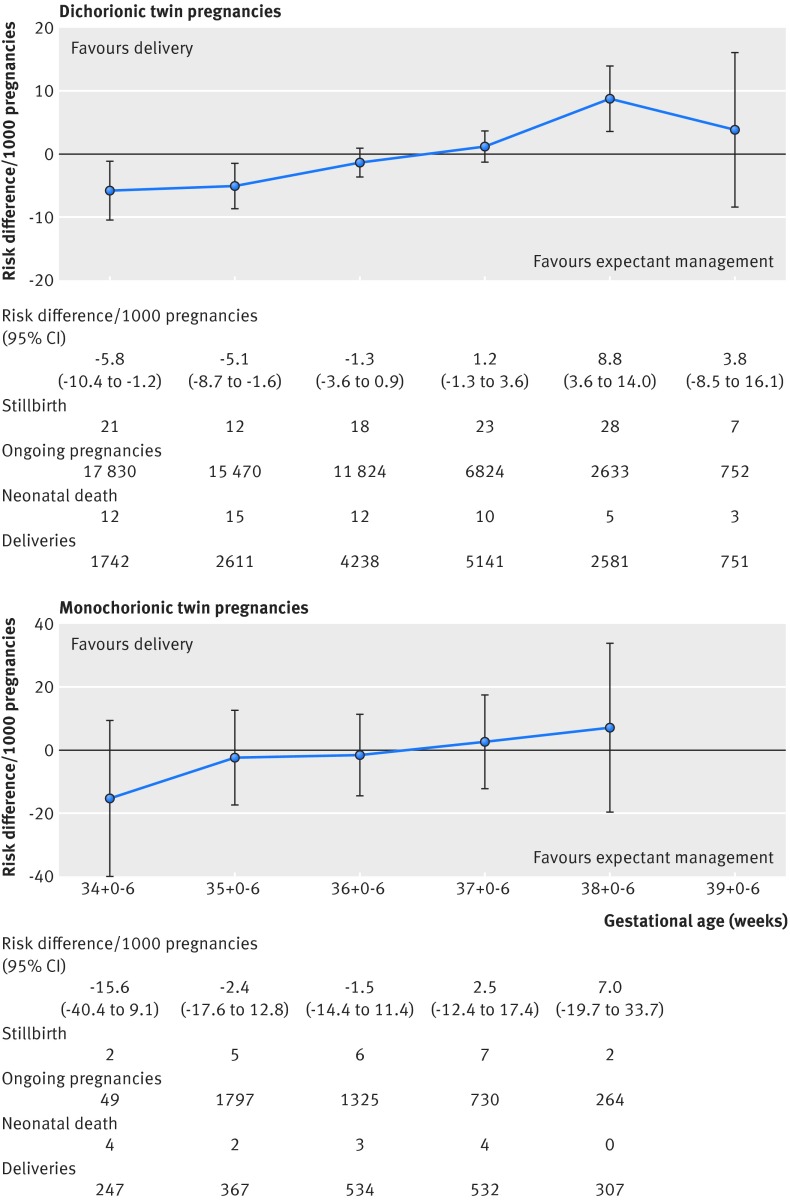
Results: 32 studies (29 685 dichorionic, 5486 monochorionic pregnancies) were included. In dichorionic twin pregnancies beyond 34 weeks (15 studies, 17 830 pregnancies), the prospective weekly risk of stillbirths from expectant management and the risk of neonatal death from delivery were balanced at 37 weeks' gestation (risk difference 1.2/1000, 95% confidence interval -1.3 to 3.6; I(2)=0%). Delay in delivery by a week (to 38 weeks) led to an additional 8.8 perinatal deaths per 1000 pregnancies (95% confidence interval 3.6 to 14.0/1000; I(2)=0%) compared with the previous week. In monochorionic pregnancies beyond 34 weeks (13 studies, 2149 pregnancies), there was a trend towards an increase in stillbirths compared with neonatal deaths after 36 weeks, with an additional 2.5 per 1000 perinatal deaths, which was not significant (-12.4 to 17.4/1000; I(2)=0%). The rates of neonatal morbidity showed a consistent reduction with increasing gestational age in monochorionic and dichorionic pregnancies, and admission to the neonatal intensive care unit was the commonest neonatal complication. The actual risk of stillbirth near term might be higher than reported estimates because of the policy of planned delivery in twin pregnancies.
Conclusions: To minimise perinatal deaths, in uncomplicated dichorionic twin pregnancies delivery should be considered at 37 weeks' gestation; in monochorionic pregnancies delivery should be considered at 36 weeks.
Systematic review registration: PROSPERO CRD42014007538.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Peter C, Wenzlaff P, Kruempelmann J, Alzen G, Bueltmann E. Perinatal morbidity and early neonatal mortality in twin pregnancies. Open J Obstet Gynecol 2013;3:78-8910.4236/ojog.2013.31017. - DOI
-
- Ortibus E, Lopriore E, Deprest J, et al. The pregnancy and long-term neurodevelopmental outcome of monochorionic diamniotic twin gestations: a multicenter prospective cohort study from the first trimester onward. Am J Obstet Gynecol 2009;200:494.e1-8. 10.1016/j.ajog.2009.01.048 pmid:19375567. - DOI - PubMed
-
- Russo FM, Pozzi E, Pelizzoni F, et al. Stillbirths in singletons, dichorionic and monochorionic twins: a comparison of risks and causes. Eur J Obstet Gynecol Reprod Biol 2013;170:131-6. 10.1016/j.ejogrb.2013.06.014 pmid:23830966. - DOI - PubMed
-
- Poulter D. Multiple Births. Parliamentary business 2014; Information on the number of obstetrics claims received between 1 April 2004 and 2031 March 2014 which have involved a multiple pregnancy are set out in the following tables. http://www.parliament.uk/business/publications/written-questions-answers..., 2016.
-
- Royal Australain and New Zealand Colleges of Obstetricians and Gynaecologists. Management of monochorionic twin pregnancy. C-Obs 42.RANZCOG, 2014: 1-11.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical