

Pharmacokinetic and Pharmacodynamic Analysis of Subcutaneous Tocilizumab in Patients With Rheumatoid Arthritis From 2 Randomized, Controlled Trials: SUMMACTA and BREVACTA
- PMID: 27599663
- PMCID: PMC5363244
- DOI: 10.1002/jcph.826
Pharmacokinetic and Pharmacodynamic Analysis of Subcutaneous Tocilizumab in Patients With Rheumatoid Arthritis From 2 Randomized, Controlled Trials: SUMMACTA and BREVACTA
Abstract
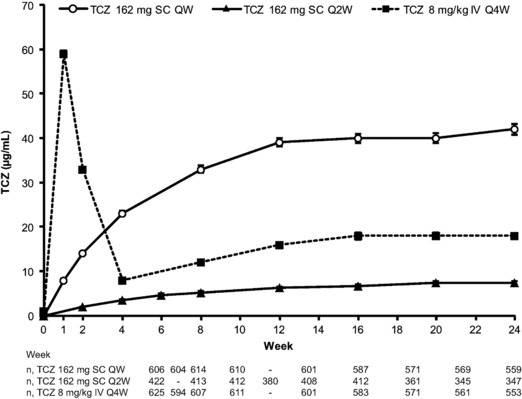
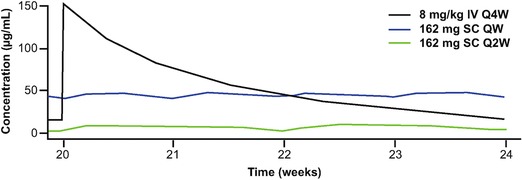
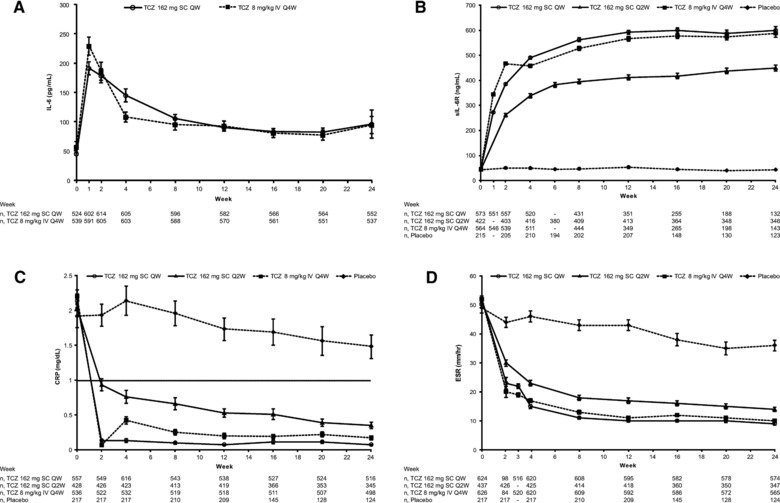
Tocilizumab is a humanized anti-interleukin-6 receptor antibody for treating rheumatoid arthritis. Pharmacokinetic/pharmacodynamic analysis was performed on the 24-week double-blind parts of 2 randomized, controlled trials: SUMMACTA and BREVACTA. SUMMACTA compared subcutaneous tocilizumab 162 mg every week to intravenous tocilizumab 8 mg/kg every 4 weeks, whereas BREVACTA evaluated 162 mg subcutaneous tocilizumab every 2 weeks versus placebo. In addition to noncompartmental analysis, a 2-compartment population pharmacokinetic model, with first-order absorption (for subcutaneous) and linear and Michaelis-Menten elimination was used. Mean observed steady-state predose tocilizumab concentrations in week 24 were 40 and 7.4 μg/mL for subcutaneous every-week and every-2-week dosing, respectively, and 18 μg/mL for intravenous dosing. In the population PK model, body weight was an important covariate affecting clearance and volume of distribution. Mean ± SD population-predicted predose concentration for patients ≥100 kg was 23.0 ± 13.5 μg/mL for subcutaneous tocilizumab every week and 1.0 ± 1.6 μg/mL for every 2 weeks. Efficacy was lowest with subcutaneous every-2-week dosing in patients > 100 kg, reflecting lower exposure. The subcutaneous every-2-week regimen is not recommended for these patients. Pharmacodynamic responses were comparable for the every-week subcutaneous and every-4-week intravenous regimens and less pronounced with the every-2-week subcutaneous regimen. No trend was observed for increased adverse events with increasing tocilizumab exposure. The results of this analysis are consistent with the noninferiority of efficacy of the every-week subcutaneous regimen to the every-4-week intravenous regimen and the superiority of the every-2-week subcutaneous regimen to placebo. These results support the label recommendations for subcutaneous dosing of tocilizumab in rheumatoid arthritis patients.
Keywords: pharmacokinetics; rheumatoid arthritis; subcutaneous; tocilizumab.
© 2016, The Authors. The Journal of Clinical Pharmacology published by Wiley Periodicals, Inc. on behalf of American College of Clinical Pharmacology.
Figures
References
-
- Gartlehner G, Hansen RA, Jonas BL, Thieda P, Lohr KN. The comparative efficacy and safety of biologics for the treatment of rheumatoid arthritis: a systematic review and metaanalysis. J Rheumatol. 2006;33(12):2398–2408. - PubMed
-
- Scott DL. Biologics‐based therapy for the treatment of rheumatoid arthritis. Clin Pharmacol Ther. 2012;91(1):30–43. - PubMed
-
- Mihara M, Kasutani K, Okazaki M, et al. Tocilizumab inhibits signal transduction mediated by both mIL‐6R and sIL‐6R, but not by the receptors of other members of IL‐6 cytokine family. Int Immunopharmacol. 2005;5(12):1731–1740. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
