

Natriuretic peptides and integrated risk assessment for cardiovascular disease: an individual-participant-data meta-analysis
- PMID: 27599814
- PMCID: PMC5035346
- DOI: 10.1016/S2213-8587(16)30196-6
Natriuretic peptides and integrated risk assessment for cardiovascular disease: an individual-participant-data meta-analysis
Abstract
Background: Guidelines for primary prevention of cardiovascular diseases focus on prediction of coronary heart disease and stroke. We assessed whether or not measurement of N-terminal-pro-B-type natriuretic peptide (NT-proBNP) concentration could enable a more integrated approach than at present by predicting heart failure and enhancing coronary heart disease and stroke risk assessment.
Methods: In this individual-participant-data meta-analysis, we generated and harmonised individual-participant data from relevant prospective studies via both de-novo NT-proBNP concentration measurement of stored samples and collection of data from studies identified through a systematic search of the literature (PubMed, Scientific Citation Index Expanded, and Embase) for articles published up to Sept 4, 2014, using search terms related to natriuretic peptide family members and the primary outcomes, with no language restrictions. We calculated risk ratios and measures of risk discrimination and reclassification across predicted 10 year risk categories (ie, <5%, 5% to <7·5%, and ≥7·5%), adding assessment of NT-proBNP concentration to that of conventional risk factors (ie, age, sex, smoking status, systolic blood pressure, history of diabetes, and total and HDL cholesterol concentrations). Primary outcomes were the combination of coronary heart disease and stroke, and the combination of coronary heart disease, stroke, and heart failure.
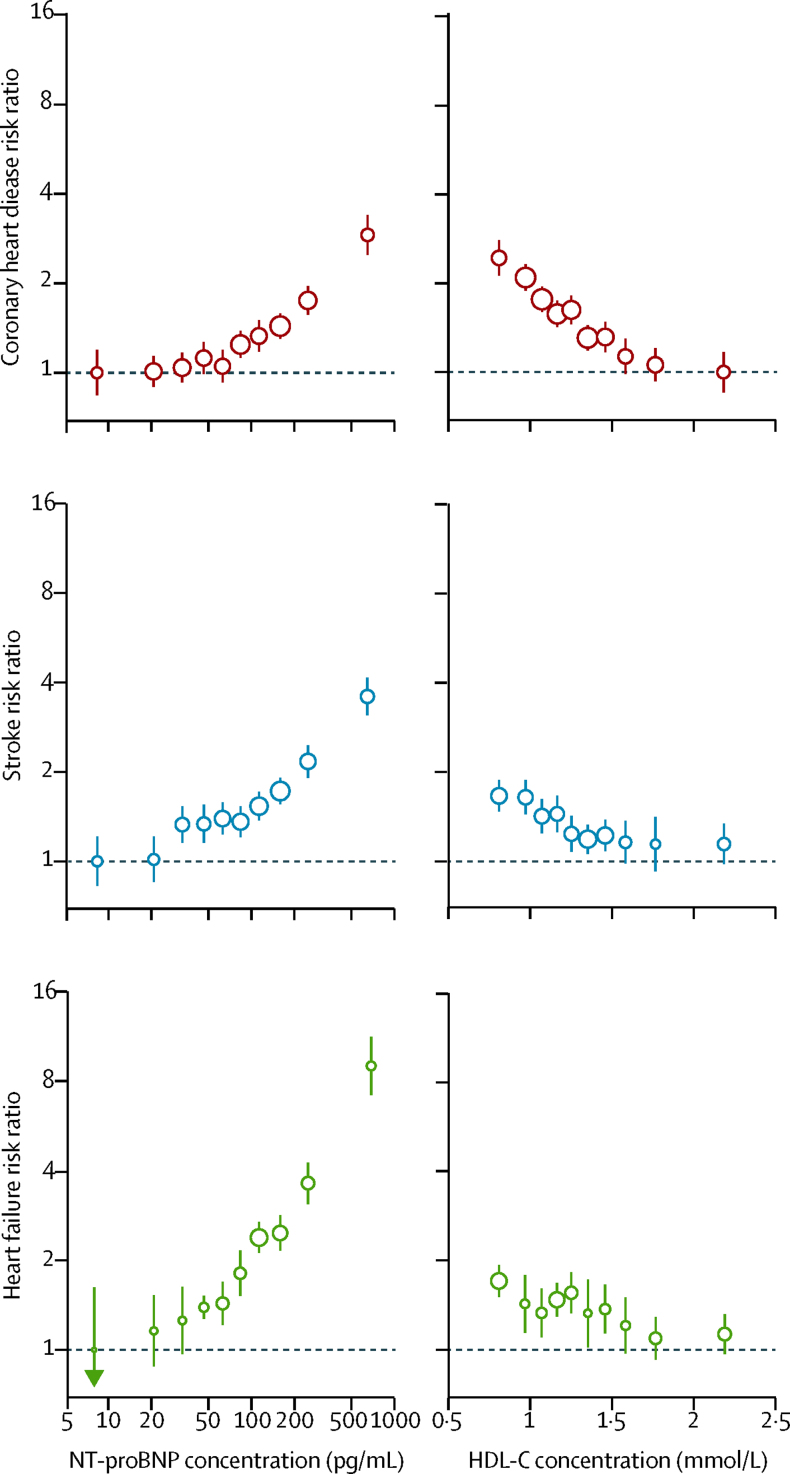
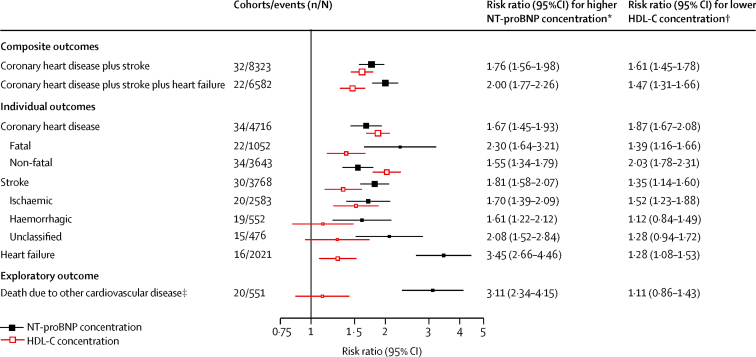
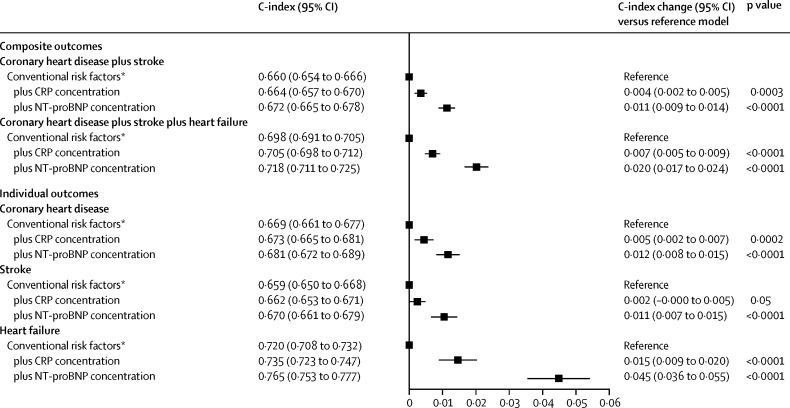
Findings: We recorded 5500 coronary heart disease, 4002 stroke, and 2212 heart failure outcomes among 95 617 participants without a history of cardiovascular disease in 40 prospective studies. Risk ratios (for a comparison of the top third vs bottom third of NT-proBNP concentrations, adjusted for conventional risk factors) were 1·76 (95% CI 1·56-1·98) for the combination of coronary heart disease and stroke and 2·00 (1·77-2·26) for the combination of coronary heart disease, stroke, and heart failure. Addition of information about NT-proBNP concentration to a model containing conventional risk factors was associated with a C-index increase of 0·012 (0·010-0·014) and a net reclassification improvement of 0·027 (0·019-0·036) for the combination of coronary heart disease and stroke and a C-index increase of 0·019 (0·016-0·022) and a net reclassification improvement of 0·028 (0·019-0·038) for the combination of coronary heart disease, stroke, and heart failure.
Interpretation: In people without baseline cardiovascular disease, NT-proBNP concentration assessment strongly predicted first-onset heart failure and augmented coronary heart disease and stroke prediction, suggesting that NT-proBNP concentration assessment could be used to integrate heart failure into cardiovascular disease primary prevention.
Funding: British Heart Foundation, Austrian Science Fund, UK Medical Research Council, National Institute for Health Research, European Research Council, and European Commission Framework Programme 7.
Copyright © 2016 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures

Comment in
-
Cardiac natriuretic peptides in plasma: from prediction to precision medicine.Lancet Diabetes Endocrinol. 2016 Oct;4(10):803-5. doi: 10.1016/S2213-8587(16)30221-2. Epub 2016 Sep 3. Lancet Diabetes Endocrinol. 2016. PMID: 27599813 No abstract available.
References
-
- Goff DC, Jr, Lloyd-Jones DM, Bennett G. 2013 ACC/AHA guideline on the assessment of cardiovascular risk. Circulation. 2014;129(25 suppl 2):S49–S73. - PubMed
-
- Greenland P, Alpert JS, Beller GA. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults. Circulation. 2010;122:e584–e636. - PubMed
-
- National Institute for Health and Care Excellence . Cardiovascular disease: risk assessment and reduction, including lipid modification. National Institute for Health and Care Excellence; London: 2014. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- SP/09/002/BHF_/British Heart Foundation/United Kingdom
- G0800270/MRC_/Medical Research Council/United Kingdom
- RG/08/014/24067/BHF_/British Heart Foundation/United Kingdom
- FS/10/37/28413/BHF_/British Heart Foundation/United Kingdom
- FS/12/62/29889/BHF_/British Heart Foundation/United Kingdom
- MR/L003120/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_00002/7/MRC_/Medical Research Council/United Kingdom
- J 3679/FWF_/Austrian Science Fund FWF/Austria
- WT_/Wellcome Trust/United Kingdom
- PG/13/66/30442/BHF_/British Heart Foundation/United Kingdom
- RG/13/13/30194/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
