

Outcome and predictors for successful resuscitation in the emergency room of adult patients in traumatic cardiorespiratory arrest
- PMID: 27600396
- PMCID: PMC5013586
- DOI: 10.1186/s13054-016-1463-6
Outcome and predictors for successful resuscitation in the emergency room of adult patients in traumatic cardiorespiratory arrest
Abstract
Background: Data of the TraumaRegister DGU® were analyzed to derive survival rates, neurological outcome and prognostic factors of patients who had suffered traumatic cardiac arrest in the early treatment phase.
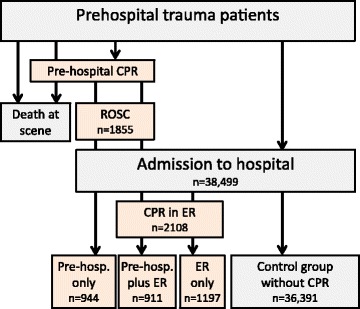
Methods: The database of the TraumaRegister DGU® from 2002 to 2013 was analyzed. The main focus of this survey was on different time points of performed resuscitation. Descriptive and multivariate analyses (logistic regression) were performed with the neurological outcome (Glasgow Outcome Scale) and survival rate as the target variable. Patients were classified according to CPR in the prehospital phase and/or in the emergency room (ER). Patients without CA served as a control group. The database does not include patients who required prehospital CPR but did not achieve ROSC.
Results: A total of 3052 patients from a total of 38,499 cases had cardiac arrest during the early post-trauma phase and required CPR in the prehospital phase and/or in the ER. After only prehospital resuscitation (n = 944) survival rate was 31.7 %, and 14.7 % had a good/moderate outcome. If CPR was required in the ER only (n = 1197), survival rate was 25.6 %, with a good/moderate outcome in 19.2 % of cases. A total of 4.8 % in the group with preclinical and ER resuscitation survived, and just 2.7 % had a good or moderate outcome. Multivariate logistic regression analysis revealed the following prognostic factors for survival after traumatic cardiac arrest: prehospital CPR, shock, coagulopathy, thorax drainage, preclinical catecholamines, unconsciousness, and injury severity (Injury Severity Score).
Conclusions: With the knowledge that prehospital resuscitated patients who not reached the hospital could not be included, CPR after severe trauma seems to yield a better outcome than most studies have reported, and appears to be more justified than the current guidelines would imply. Preclinical resuscitation is associated with a higher survival rate and better neurological outcome compared with resuscitation in the ER. If resuscitation in the ER is necessary after a preclinical performed resuscitation the survival rate is marginal, even though 56 % of these patients had a good and moderate outcome. The data we present may support algorithms for resuscitation in the future.
Figures
References
-
- Cera SM, et al. Physiologic predictors of survival in post-traumatic arrest. Am Surg. 2003;69(2):140–4. - PubMed
-
- Yanagawa Y, et al. Experience of treatment for blunt traumatic out-of-hospital cardiopulmonary arrest patients over 24 years: head injury v.s. non-head injury. No Shinkei Geka. 2004;32(3):231–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
