Juvenile nasopharyngeal angiofibroma
- PMID: 27601836
- PMCID: PMC4989574
- DOI: 10.4103/0973-029X.185908
Juvenile nasopharyngeal angiofibroma
Abstract
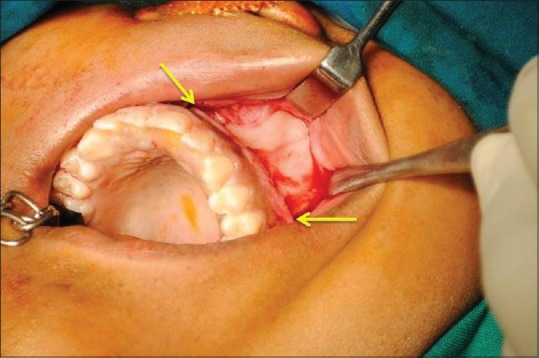
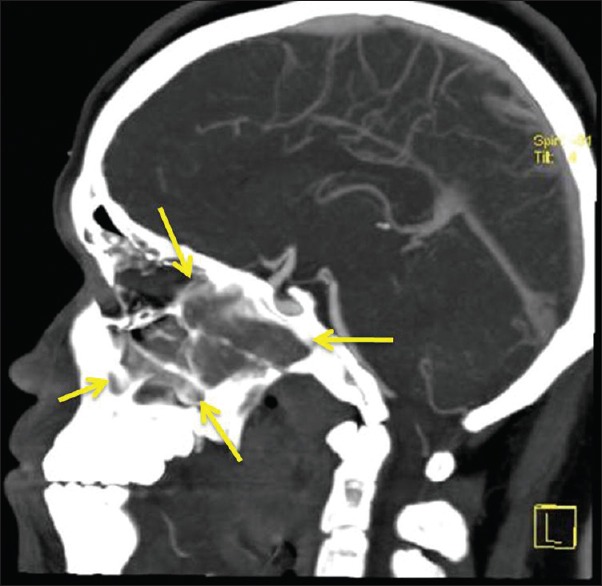
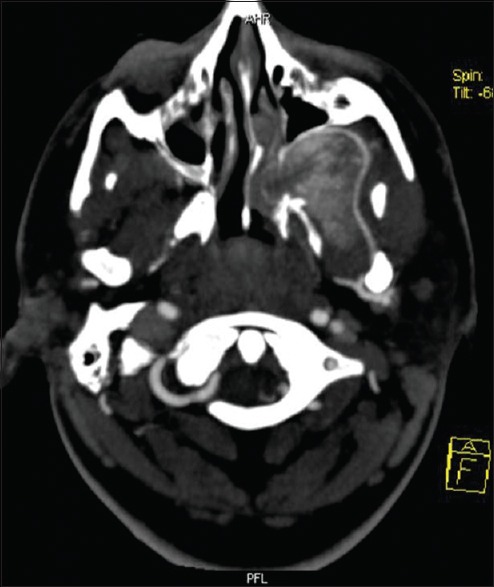
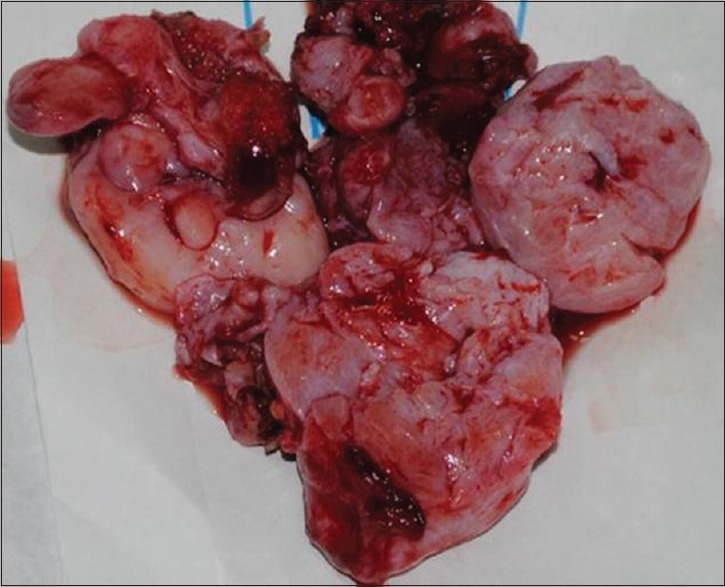
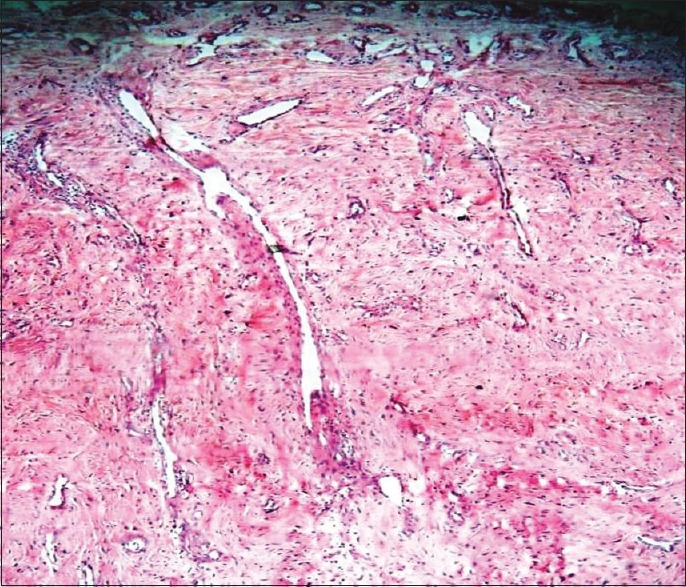
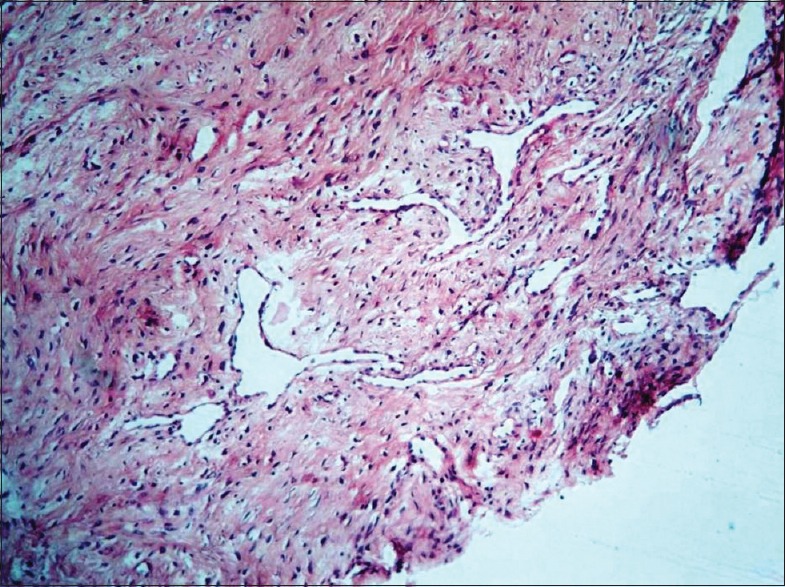
Juvenile nasopharyngeal angiofibroma (JNA) is a rare benign tumor arising predominantly in the nasopharynx of adolescent males. It is an aggressive neoplasm and shows a propensity for destructive local spread often extending to the base of the skull and into the cranium. Clinically, however, it is obscure with painless, progressive unilateral nasal obstruction being the common presenting symptom with or without epistaxis and rhinorrhea. Diagnosis of JNA is made by complete history, clinical examination, radiography, nasal endoscopy and by using specialized imaging techniques such as arteriography, computer tomography and magnetic resonance imaging. Histopathology reveals a fibrocellular stroma with spindle cells and haphazard arrangement of collagen interspersed with an irregular vascular pattern. A case report of JNA with rare intra-oral manifestation in a 17-year-old male patient is presented in the article. JNA being an aggressive tumor may recur posttreatment. Thus, early diagnosis, accurate staging, and adequate treatment are essential in the management of this lesion.
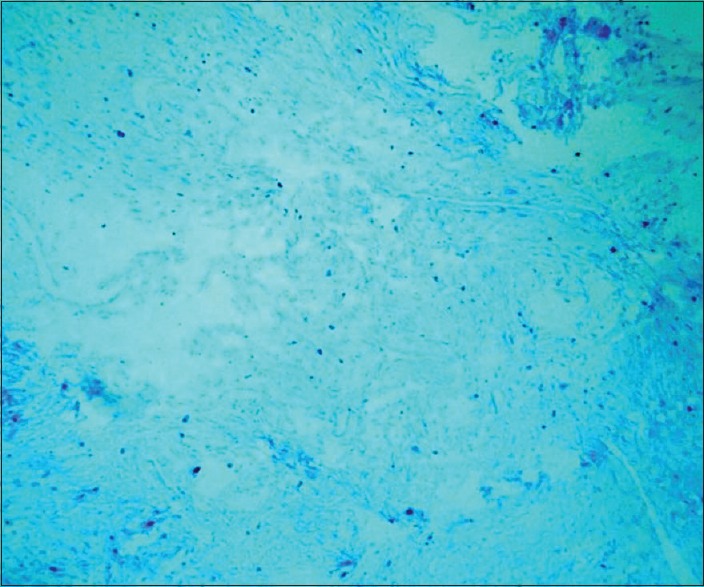
Keywords: Androgen receptor; juvenile angiofiborma; nasopharyngeal angiofibroma.
Figures
References
-
- Coutinho-Camillo CM, Brentani MM, Nagai MA. Genetic alterations in juvenile nasopharyngeal angiofibromas. Head Neck. 2008;30:390–400. - PubMed
-
- Biswas D, Saha S, Bera SP. Relative distribution of the tumours of ear, nose and throat in the paediatric patients. Int J Pediatr Otorhinolaryngol. 2007;71:801–5. - PubMed
-
- Schick B, Rippel C, Brunner C, Jung V, Plinkert PK, Urbschat S. Numerical sex chromosome aberrations in juvenile angiofibromas: Genetic evidence for an androgen-dependent tumor? Oncol Rep. 2003;10:1251–5. - PubMed
-
- Yi Z, Fang Z, Lin G, Lin C, Xiao W, Li Z, et al. Nasopharyngeal angiofibroma: A concise classification system and appropriate treatment options. Am J Otolaryngol. 2013;34:133–41. - PubMed
-
- Zhang M, Sun X, Yu H, Hu L, Wang D. Biological distinctions between juvenile nasopharyngeal angiofibroma and vascular malformation: An immunohistochemical study. Acta Histochem. 2011;113:626–30. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources