

Management of pain in chronic pancreatitis with emphasis on exogenous pancreatic enzymes
- PMID: 27602238
- PMCID: PMC4986390
- DOI: 10.4292/wjgpt.v7.i3.370
Management of pain in chronic pancreatitis with emphasis on exogenous pancreatic enzymes
Abstract
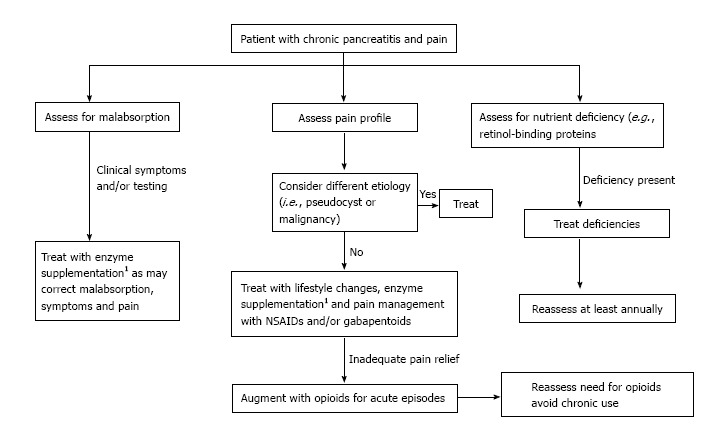
One of the most challenging issues arising in patients with chronic pancreatitis is the management of abdominal pain. Many competing theories exist to explain pancreatic pain including ductal hypertension from strictures and stones, increased interstitial pressure from glandular fibrosis, pancreatic neuritis, and ischemia. This clinical problem is superimposed on a background of reduced enzyme secretion and altered feedback mechanisms. Throughout history, investigators have used these theories to devise methods to combat chronic pancreatic pain including: Lifestyle measures, antioxidants, analgesics, administration of exogenous pancreatic enzymes, endoscopic drainage procedures, and surgical drainage and resection procedures. While the value of each modality has been debated over the years, pancreatic enzyme therapy remains a viable option. Enzyme therapy restores active enzymes to the small bowel and targets the altered feedback mechanism that lead to increased pancreatic ductal and tissue pressures, ischemia, and pain. Here, we review the mechanisms and treatments for chronic pancreatic pain with a specific focus on pancreatic enzyme replacement therapy. We also discuss different approaches to overcoming a lack of clinical response update ideas for studies needed to improve the clinical use of pancreatic enzymes to ameliorate pancreatic pain.
Keywords: Chronic pancreatitis; Clinical trials; Fat malabsorption; Pain; Pancreatic enzyme replacement therapy; Pancreatic insufficiency; Protease; Trypsin.
Figures
Similar articles
-
Surgical treatment of chronic pancreatitis and quality of life after operation.Surg Clin North Am. 1999 Aug;79(4):913-44. doi: 10.1016/s0039-6109(05)70051-7. Surg Clin North Am. 1999. PMID: 10470335 Review.
-
[Recent Advances in Management of Chronic Pancreatitis].Korean J Gastroenterol. 2015 Sep;66(3):144-9. doi: 10.4166/kjg.2015.66.3.144. Korean J Gastroenterol. 2015. PMID: 26387696 Review. Korean.
-
[Medical and endoscopic treatment of chronic pancreatitis].Rev Prat. 1996 Mar 15;46(6):715-21. Rev Prat. 1996. PMID: 8731739 Review. French.
-
Pancreatic exocrine insufficiency: diagnostic evaluation and replacement therapy with pancreatic enzymes.Dig Dis. 2010;28(2):339-43. doi: 10.1159/000319411. Epub 2010 Sep 1. Dig Dis. 2010. PMID: 20814209 Review.
-
Conservative treatment of chronic pancreatitis.Dig Dis. 2013;31(1):43-50. doi: 10.1159/000345720. Epub 2013 Jun 17. Dig Dis. 2013. PMID: 23797122 Review.
Cited by
-
Imaging of inflammatory disease of the pancreas.Br J Radiol. 2021 Jul 1;94(1123):20201214. doi: 10.1259/bjr.20201214. Epub 2021 Jun 11. Br J Radiol. 2021. PMID: 34111970 Free PMC article. Review.
-
Rational Use of Pancreatic Enzymes for Pancreatic Insufficiency and Pancreatic Pain.Adv Exp Med Biol. 2019;1148:323-343. doi: 10.1007/978-981-13-7709-9_14. Adv Exp Med Biol. 2019. PMID: 31482505 Free PMC article. Review.
-
The influence of erythropoietin on apoptosis and fibrosis in the early phase of chronic pancreatitis in rats.Arch Med Sci. 2020 Oct 12;17(4):1100-1108. doi: 10.5114/aoms.2020.99800. eCollection 2021. Arch Med Sci. 2020. PMID: 34336038 Free PMC article.
-
Piperine ameliorates the severity of fibrosis via inhibition of TGF‑β/SMAD signaling in a mouse model of chronic pancreatitis.Mol Med Rep. 2019 Oct;20(4):3709-3718. doi: 10.3892/mmr.2019.10635. Epub 2019 Sep 2. Mol Med Rep. 2019. PMID: 31485676 Free PMC article.
-
Anterograde Endoscopic Ultrasound-Guided Pancreatic Duct Drainage: A Technical Review.Dig Dis Sci. 2019 Jul;64(7):1770-1781. doi: 10.1007/s10620-019-05495-9. Epub 2019 Feb 7. Dig Dis Sci. 2019. PMID: 30734236 Review.
References
-
- Howard JM, Hess W. New York: Kluwer Adademic/Plenum Publishers; 2002. History of the pancreas: Mysteries of a hidden organ.
-
- Johnston GW. Calculous and other affections of the pancreatic ducts. Am J Med Sci. 1883;86:404–429.
-
- Singer MV, Gyr K, Sarles H. Revised classification of pancreatitis. Report of the Second International Symposium on the Classification of Pancreatitis in Marseille, France, March 28-30, 1984. Gastroenterology. 1985;89:683–685. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
